Background: Hemolysis-related renal failure has been described after pulmonary vein isolation (PVI) with pulsed-field ablation (PFA). However, it remains unknown whether risk and extend of hemolysis following PFA for the treatment of atrial fibrillation (AF) varies by platform.
Aim: This study sought to investigate the potential for hemolysis during AF ablation using a novel three-dimensional mapping platform combined with a lattice-tip catheter (Sphere-9TM, Medtronic Inc.) that can toggle between monopolar PFA and radiofrequency (RF) energy delivery (AfferaTM, Medtronic Inc.).
Methods: We performed a retrospective analysis of hemolysis parameters among consecutive patients undergoing AF ablation using the Affera mapping and ablation system in combination with the Sphere-9 catheter. Hemolysis markers were assessed immediately before and the day after the procedure.
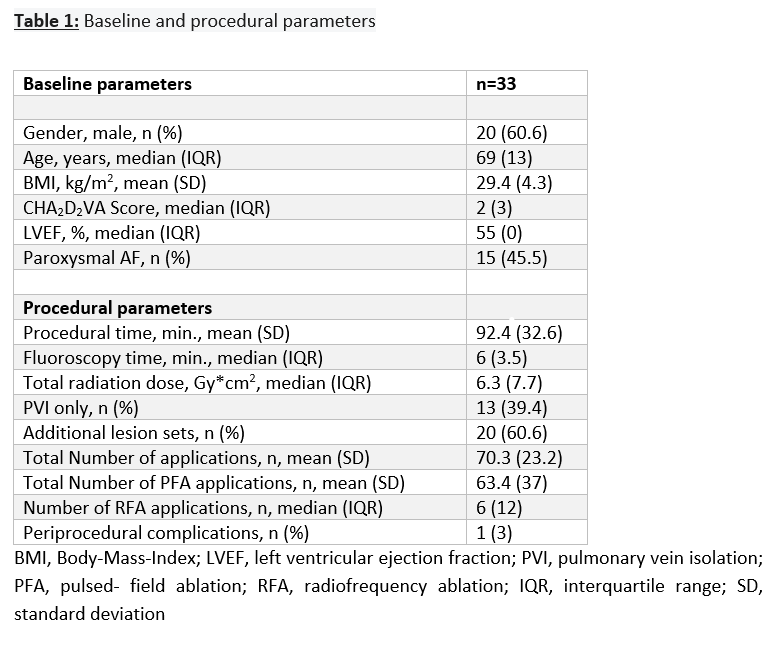
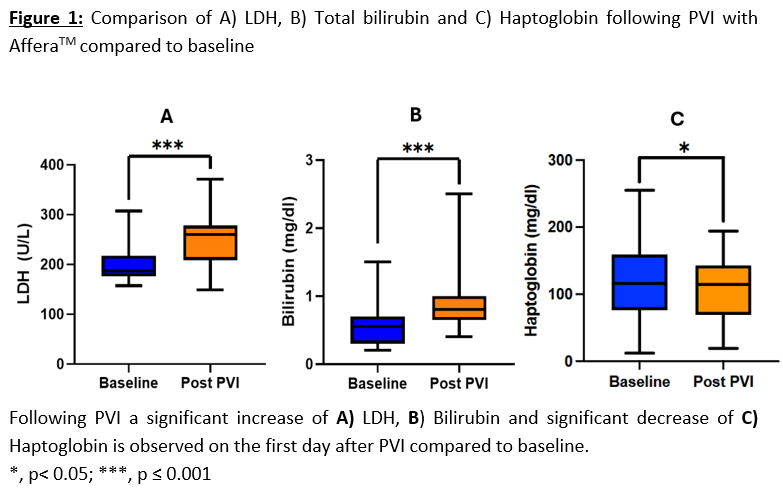
Results: A total of 33 patients (median age 69 years, 61% male, 46% suffering from paroxysmal AF) undergoing AF ablation were analyzed, including 20 (61%) reablation procedures. Mean total number of applications and mean number of PFA-applications was 70 ± 23 and 63± 37 (Table 1). A significant increase in lactatdehydrogenase (LDH) levels by 78.5% (197 ± 33 vs. 251 ± 51 U/L, p<0.001), total bilirubin levels by 73.8% (0.59 ± 0.35 vs. 0.8 ± 0.3 mg/dl, p<0.001), direct bilirubin levels by 49.2 % (0.3 ± 0.23 vs. 0.49 ± 0.61 mg/dl, p=0.03) and decrease in haptoglobin levels by 10.8% (120 ± 53.3 vs. 107 ± 46.3 mg/dl, p=0.023) was documented within 24 hours after the procedure compared to baseline (Figure 1). No significant changes in creatinine levels (1.02 ± 0.3 vs. 0.98 ± 0.29 mg/dl, p= 0.064), as an indicator of renal failure, were observed after the procedure. Hemolysis parameters did not correlate significantly with the total number of PFA applications (∆Haptoglobin mg/dl, r=0.2, p=0.31; ∆Bilirubin mg/dl, r=0.22, p=0.26; ∆LDH U/L, r=0.05, p=0.81).
Conclusion: Hemolysis after PFA is a frequent finding and seems to occur regardless of platform and PFA waveform used. However, in our cohort, no renal failure was noted.