Background:
Epicardial ventricular tachycardia (VT) ablation is a therapeutic option for drug-refractory VT, particularly when endocardial ablation fails or is inadequate. However, accurately identifying patients who will benefit most from an epicardial approach remains challenging due to its higher procedure-related risks.
Objective:
This study aimed to develop and validate a predictive scoring model — EPI-VT-Score — to identify patients likely to benefit from epicardial VT ablation.
Methods:
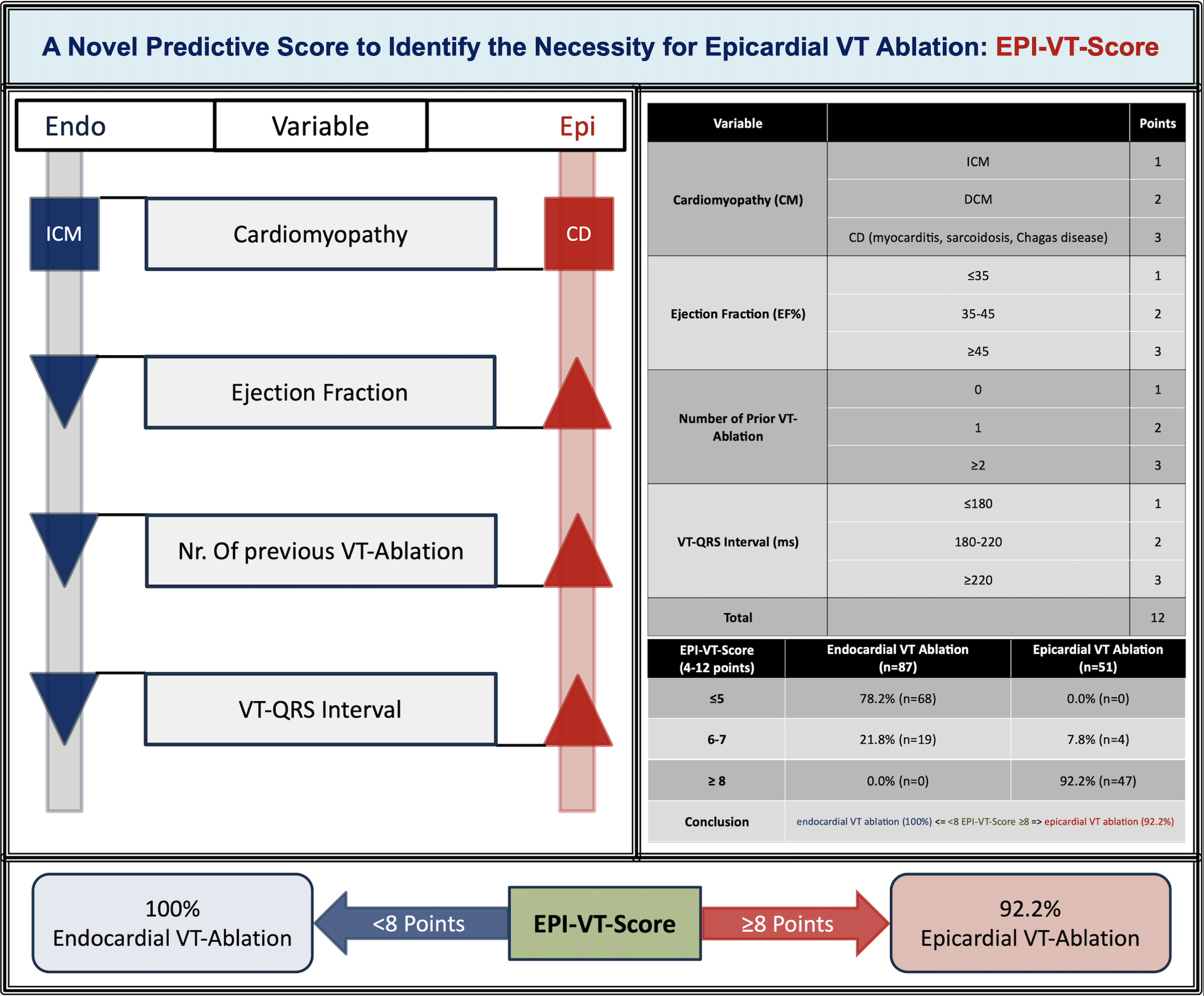
We retrospectively analyzed data from 138 patients (mean age 64.9±11.3 years, 89.9% male) who underwent VT ablation between 2018 and 2024. Four predictors — underlying cardiomyopathy, left ventricular ejection fraction (LVEF), number of prior VT ablations, and VT-QRS interval — were identified and incorporated into the EPI-VT-Score, which ranges from 4 to 12 points (Figure 1). Score performance was assessed using area under curve (AUC).
Results:
Among 138 patients, 51 (37.0%) underwent epicardial ablation. The EPI-VT-Score accurately predicted epicardial ablation necessity with an AUC of 0.990 (95% CI, 0.978–1.000). A score ≥8 identified epicardial need with 92.2% sensitivity and 100% specificity. Patients scoring <8 were effectively managed with endocardial-only ablation.
Conclusion:
The EPI-VT-Score can be a clinical support to evaluate preprocedural necessity for epicardial access and the complexity of the procedure to improves procedural outcomes as well as minimize unnecessary procedural risks.
Figure 1: