*the two authors on first position and the two authors on last position contributed equally
Objective:
Previous studies have demonstrated that biventricular (BiV) pacing is associated with less progression—and even improvement—of mitral regurgitation (MR) compared to right ventricular (RV) pacing (Scott et al., Circulation, 2010). Respective work is 15 years old, and it is unclear if changes in techniques and material may have influenced this observation. Therefore, we aimed to examine the influence of BiV and right ventricular (RV) pacing on MR in a more recent cohort.
Methods:
We performed a retrospective analysis of 549 patients who received a pacemaker (PM), implantable cardioverter defibrillator (ICD), or cardiac resynchronization therapy (CRT) device at our institution between 2010 and 2016, all of whom had complete follow-up including device interrogation and transthoracic echocardiography at one and three years. Patients were grouped according to pacing modality: RV or BiV pacing. MR severity was assessed at baseline and at follow-up, and classified as improved, worsened, or unchanged (≥1 grade difference). Statistical comparisons were performed using the Chi-Square test for categorical variables.
Results:
Median age was 68 years [IQR: 57-76], with 419 (76.3%) being male. Of these patients, 21.5% received an ICD, 30.4% a PM, and 48.1% a CRT device (RV: n = 285; BiV: n = 264). BiV patients had worse left ventricular (LV) function. At three-year follow-up, MR had decreased by one or more degrees in 28.9% of patients in the BiV group compared to only 14.3% in the RV group. Furthermore, MR had increased by one or more degrees in 27.8% of cases in the RV group (compared to 21.5 % in the BiV group). This difference met statistical significance (P < 0.001).
Conclusion:
At three-year follow-up, BiV pacing was associated with a significantly higher rate of MR improvement and a lower rate of MR progression compared to RV pacing, consistent with prior findings.
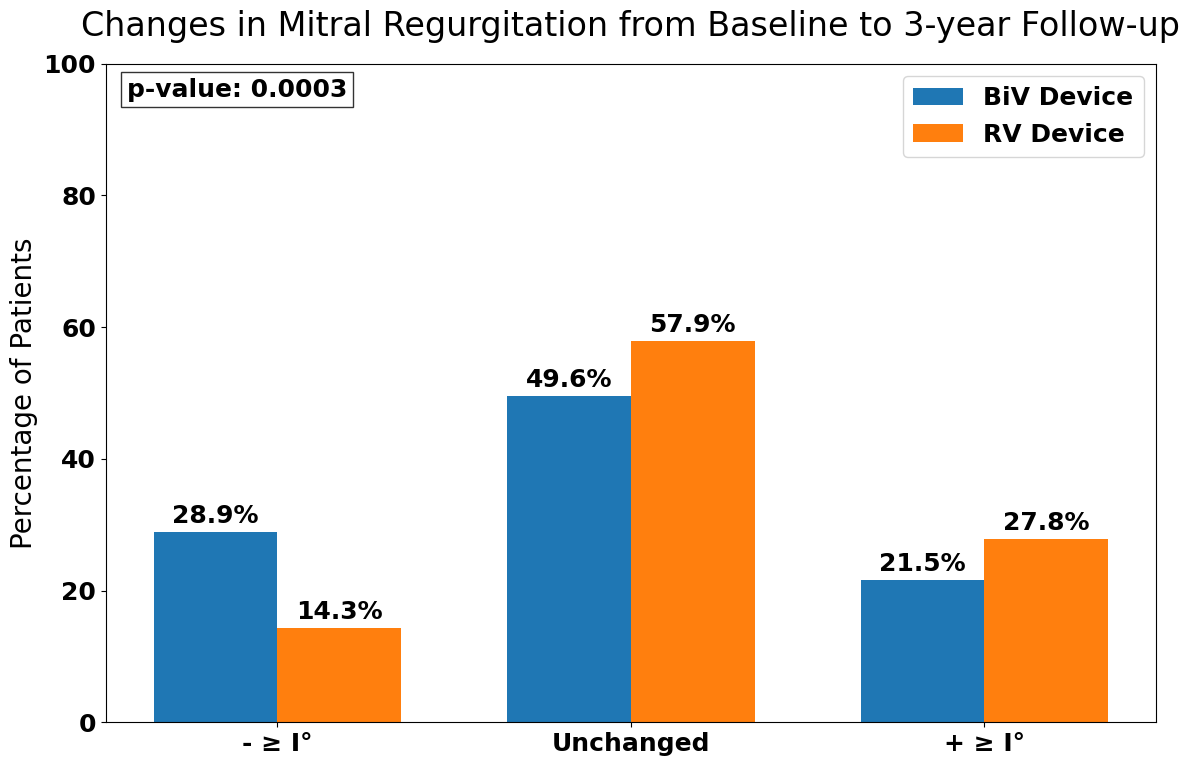
Figure 1: Changes in Mitral Regurgitation from Baseline to 3-Years Follow-Up.



