Background:Catheter ablation, the first-line treatment for atrial arrhythmia, relies on myocardial scarring for treatment success. It is currently unclear why scar formation is negatively affected in some patient groups, like patients with high BMI. Also, the early phase of post-ablation wound healing remains poorly understood and may be shaped by the patient's baseline immunological profile. This study aimed to identify circulating immune biomolecules that might influence scar formation mechanisms during the initial inflammatory response.
Methods:23 biomolecules associated with immune cell recruitment and resident cardiac immune cell populations were measured in pre-ablation plasma samples of patients undergoing catheter ablation for atrial arrhythmia (n=60): Arg1, CXCL9, EGF, GDF-15, GM CSF, IFN-, IL-1, IL-1RA, IL-2, IL-4, IL-5, IL-6, IL-10, IL-23, IL-12p40, IL-12p60, IP-10, NT proBNP, OPN, TARC, TGF-, TNF- & VEGF. Patients were grouped by arrhythmia recurrence within 24 hours post-ablation. Clinical parameters were recorded and included in multivariate analysis.
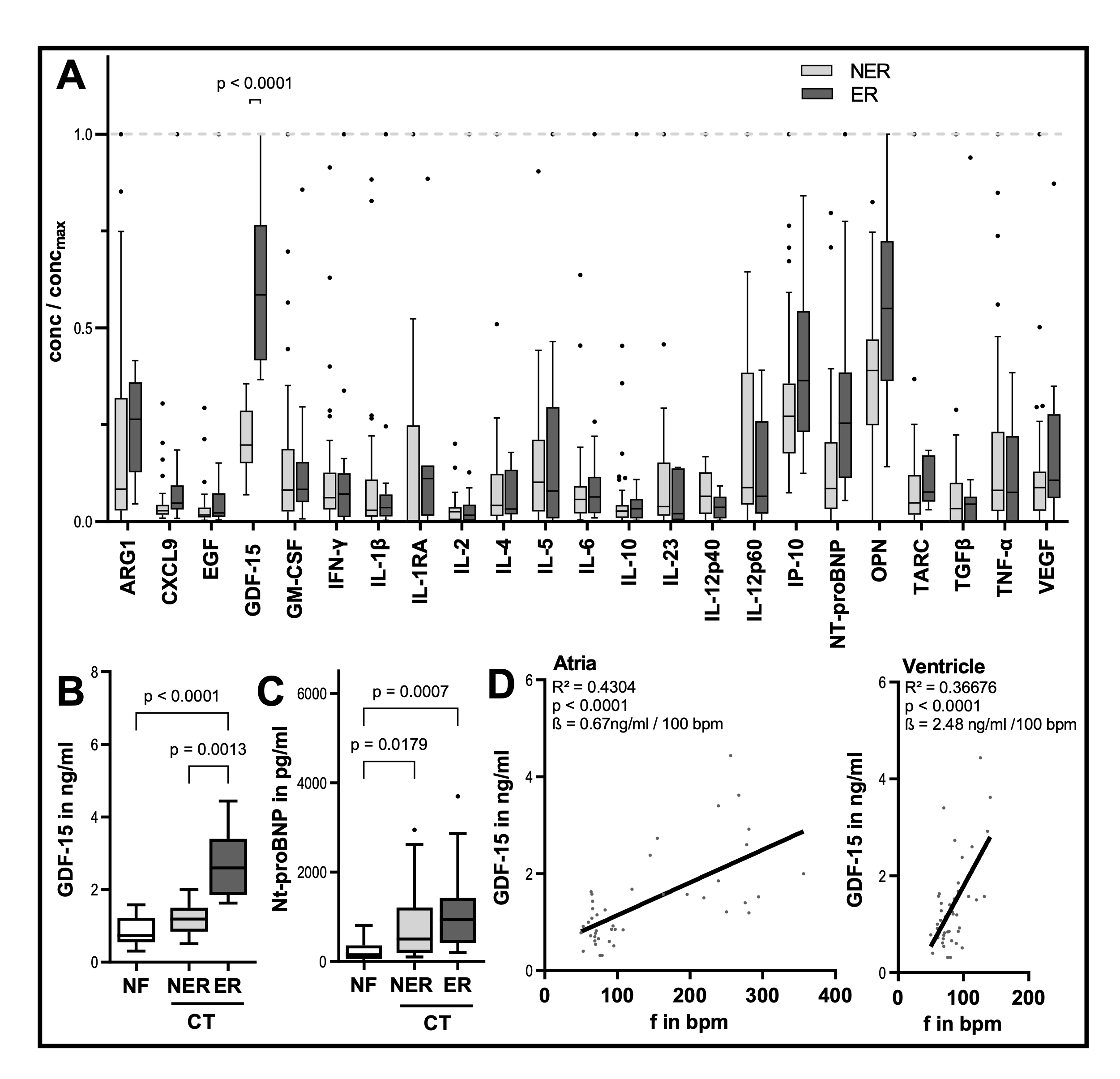
Results:24-hour ER occurred in 30% of patients (n = 18), 70% (n = 42) remained in sinus rhythm. One out of the 23 biomolecule candidates, growth/differentiation factor 15 (GDF-15), showed strict statistical correlation to ER incidence: GDF-15 prior to ablation in ER patients was 2.7 ± 0.9 ng/ml compared to 1.2 ± 0.4 ng/ml in patients without ER (p < 0.001). Incidence of 24-hour ER and the GDF-15 predictive effect were restricted to patients with chronic tachycardia (CT), normofrequent (NF) patients experienced no ER. NT-proBNP as a heart failure marker differed between NF and CT patients, but unlike GDF-15 was not predictive of ER. After adjustment for BMI, age, gender, EF, and NT-proBNP by multivariate regression, GDF-15 remained the strongest independent predictor of ER (p < 0.001). Pre-ablation GDF 15 levels were correlated to tachycardia severity, rising proportional to chamber frequencies (atrial: 0.7 ng/ml per 100 bpm; p < 0.001; ventricular: 2.5 ng/ml per 100 bpm, p < 0.001).
Discussion:Previous work has shown GDF-15 to be involved in immune cell migration, tissue repair and cardiovascular stress response. We have now identified GDF-15 as a strong statistical predictor of 24-hour recurrence after atrial ablation in chronic tachycardia. The data suggest that high GDF-15 either marks a CT patient sub-population pre-disposed for poor scar formation or that GDF 15 causally interferes with proper scar formation directly, possibly by affecting immune cell recruitment. These effects appear to be independent of traditional markers like NT-proBNP. Circulating GDF 15 is elevated in high BMI patients and multiple cardiovascular disease states, but it remains to be explored whether GDF-15 contributes to poor scar formation in these patient groups.