Background: Primary cardiac or mediastinal angiosarcomas are exceedingly rare, highly aggressive tumors that often present with nonspecific symptoms and are frequently misdiagnosed. In young, previously healthy patients, initial presentation can mimic inflammatory heart diseases such as pericarditis or myocarditis, delaying definitive diagnosis and treatment.
Case Presentation: A 22-year-old previously healthy male presented with cardiogenic shock and echocardiographically confirmed pericardial tamponade (Figure 1). Emergency pericardiocentesis drained 2.5 L of hemorrhagic fluid, and the patient was stabilized in the ICU with inotropic support. Transthoracic echocardiography revealed global left ventricular dysfunction (EF ~10%). Empiric antibiotic therapy was initiated. Cardiac MRI showed diffuse myocardial edema consistent with perimyocarditis, along with a large pericardial effusion. Endomyocardial biopsy revealed lymphocytic infiltration without eosinophils or giant cells. High-dose corticosteroids and chochizin were administered, leading to full recovery of left ventricular function. Extensive infectious workup remained negative. However, repeat cardiac MRI revealed a contrast-enhancing mediastinal mass with infiltrative growth into the right atrium and ascending aorta as well as relapse pericardial efusion. PET-CT demonstrated intense FDG uptake in the lesion, raising suspicion for malignancy (Figure 2).Subsequent targeted CT guided biopsy confirmed the diagnosis of a high-grade, undifferentiated angiosarcoma originating in the mediastinum with direct cardiac invasion. The patient was transferred to an oncology center for further management and systemic therapy planning.
Discussion: This case illustrates the diagnostic complexity of infiltrating cardio-mediastinal angiosarcoma, particularly when it mimics perimyocarditis in a young patient. Initial improvement under corticosteroids and absence of early histological malignancy markers contributed to diagnostic delay. Only multimodal imaging and targeted biopsy revealed the true malignant nature of the infiltrative process.
Conclusion: Angiosarcoma can be considered in the differential diagnosis of young patients presenting with hemorrhagic pericardial effusion and infiltrative mediastinal masses, especially when the clinical course deviates from typical inflammatory disease. Early use of advanced imaging and interdisciplinary collaboration are essential for timely diagnosis and oncologic intervention.
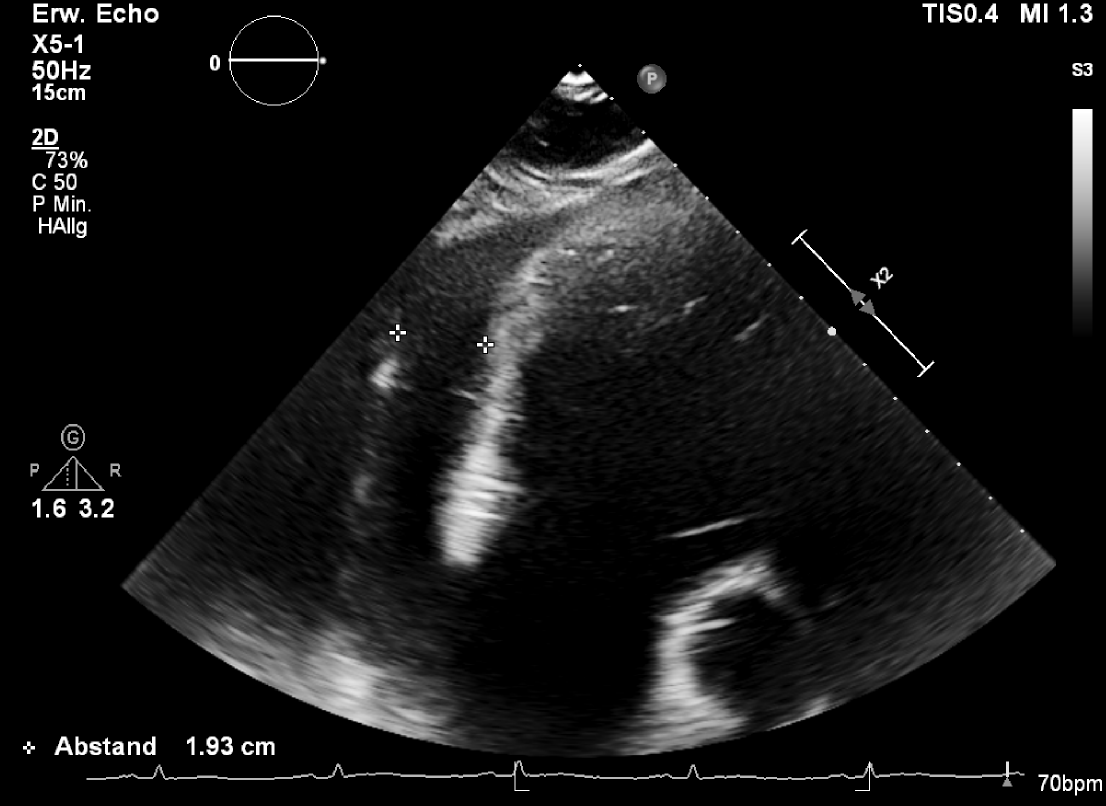
Figure 1: Transthoracic echocardiogram showing a large (1.9cm) pericardial effusion surrounding the heart.
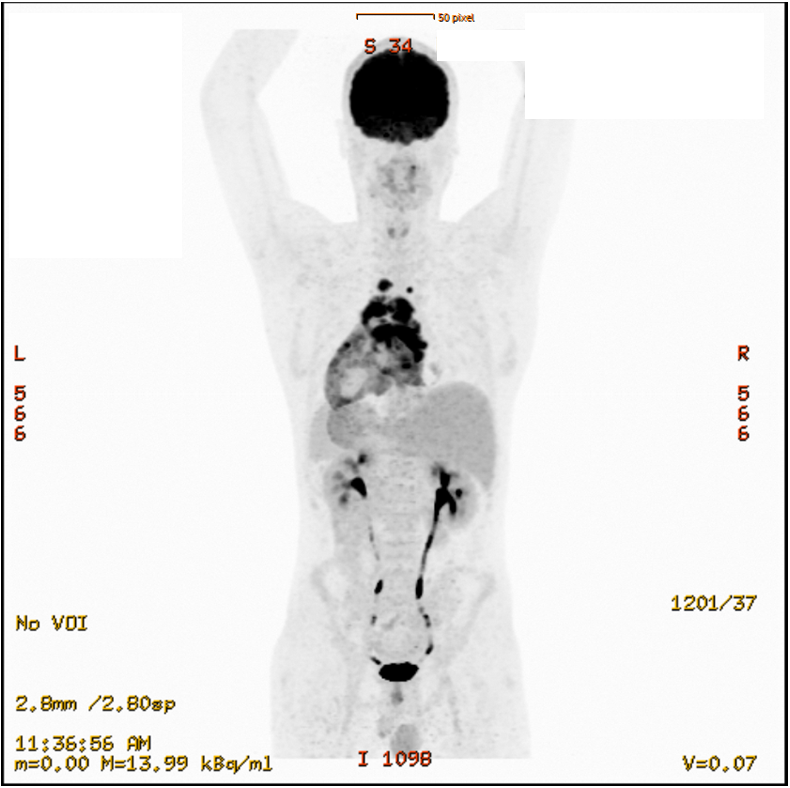
Figure 2: Fused PET/CT image demonstrating increased metabolic activity in pericardial and mediastinal structures surrounding the heart



