Background:
Atrial fibrillation (AF) occurs in up to 70% of patients with ATTR cardiac amyloidosis (CA) but is much rare in the AL type CA. Patients with CA and AF have worse outcomes and radiofrequency catheter ablation (RFCA) is associated with a high arrhythmia recurrence of 30-70%. Only limited data exist regarding left atrial (LA) und right atrial (RA) substrate in CA.
Purpose:
We assume that extensive bi-atrial amyloid depositions may explain the poorer outcomes after RFCA. This study aimed to describe the arrhythmia types and outcomes after voltage-guided bi-atrial mapping and ablation. Furthermore, we compared atrial voltage patterns in patients with light-chain (AL) and transthyretin (ATTR) cardiac amyloidosis.
Methods:
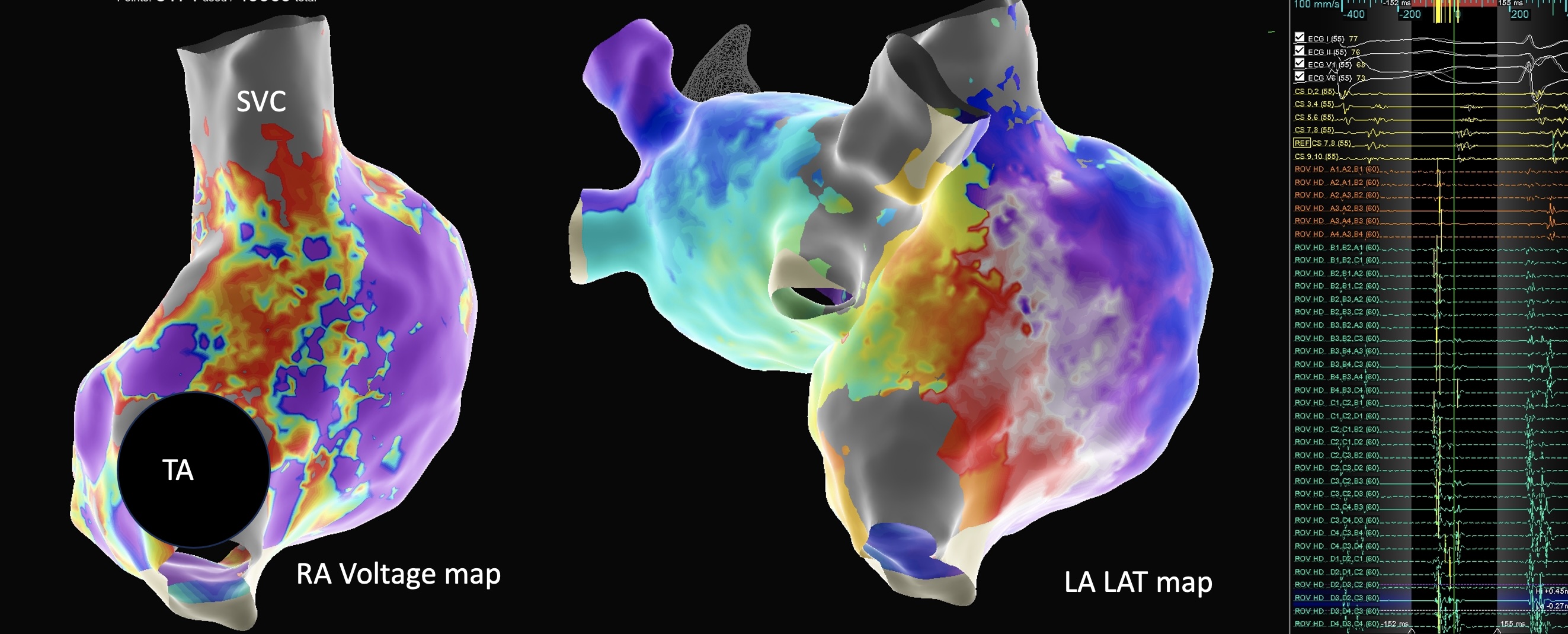
In retrospective analysis, ten patients with CA and atrial arrhythmias (nine male; age 73±6 years; EF 51±10%) were analyzed. Three had AL amyloidosis and seven had ATTR, five of them were treated with Tafamidis. Bi-atrial mapping and voltage-guided bi-atrial ablation was performed (Figure). Bipolar and unipolar voltage amplitude, distribution, as well as rhythm outcomes were analyzed.
Results:
Bipolar mapping using the threshold 0.2-0.5 mV revealed extensive bi-atrial involvement in 100% ATTR CA patients and in 0% of the AL CA patients. Bi-atrial septal involvement was the most frequent with 60%. LA unipolar voltage was 0.69 ± 0.27 mV in ATTR and 1.08 ± 0.66 mV in AL; P = 0.23; while maximal LA unipolar amplitude was 4.56 mV ± 0.82 (ATTR) versus 5.68 mV ± 1.11 (AL); P= 0.13. Pulmonary veins isolation was performed in nine patients. Cavotricuspid isthmus ablation for typical atrial flutter was performed in four and additional RA ablation in one case. After 11 (IQR 3-14) months, arrhythmia recurrences appeared in two patients (20%) in the ATTR-group.
Conclusions:
ATTR amyloidosis is characterized by extensive bi-atrial involvement and lower unipolar and bipolar signals, as compared to AL amyloidosis. Right atrial arrhythmias are frequent. Substrate-guided, bi-atrial RFCA may improve outcomes. These findings highlight the clinical relevance of tailored, substrate-based ablation strategies to optimize rhythm control in patients with cardiac amyloidosis.



