Background and aim
Large-bore thrombectomy represents an interventional treatment option for acute pulmonary embolism (PE), that mechanically aspirates thrombi from the pulmonary arteries. However, data on the relationship between the weight and volume of aspirated thrombus and clinical outcomes remain limited. There is a widespread believe, that thrombus weight and volume might contribute to severity of PE.
Methods
In this prospective, open-label study, 48 patients with acute symptomatic, computed tomography-confirmed PE and signs of right heart overload underwent large-bore thrombectomy. Right heart catheterization was performed immediately before and after thrombectomy, and again after three months. Transthoracic echocardiography was performed before thrombectomy, at discharge, and at three months. We assessed the weight and volume of aspirated thrombus and their association with baseline clinical characteristics, hemodynamic measurements, echocardiographic findings, and blood chemistry. As most variables were not normally distributed, Spearman correlations were assessed, which were corrected with Benjamin Hochberg correction for multiple exploratory testing.
Results
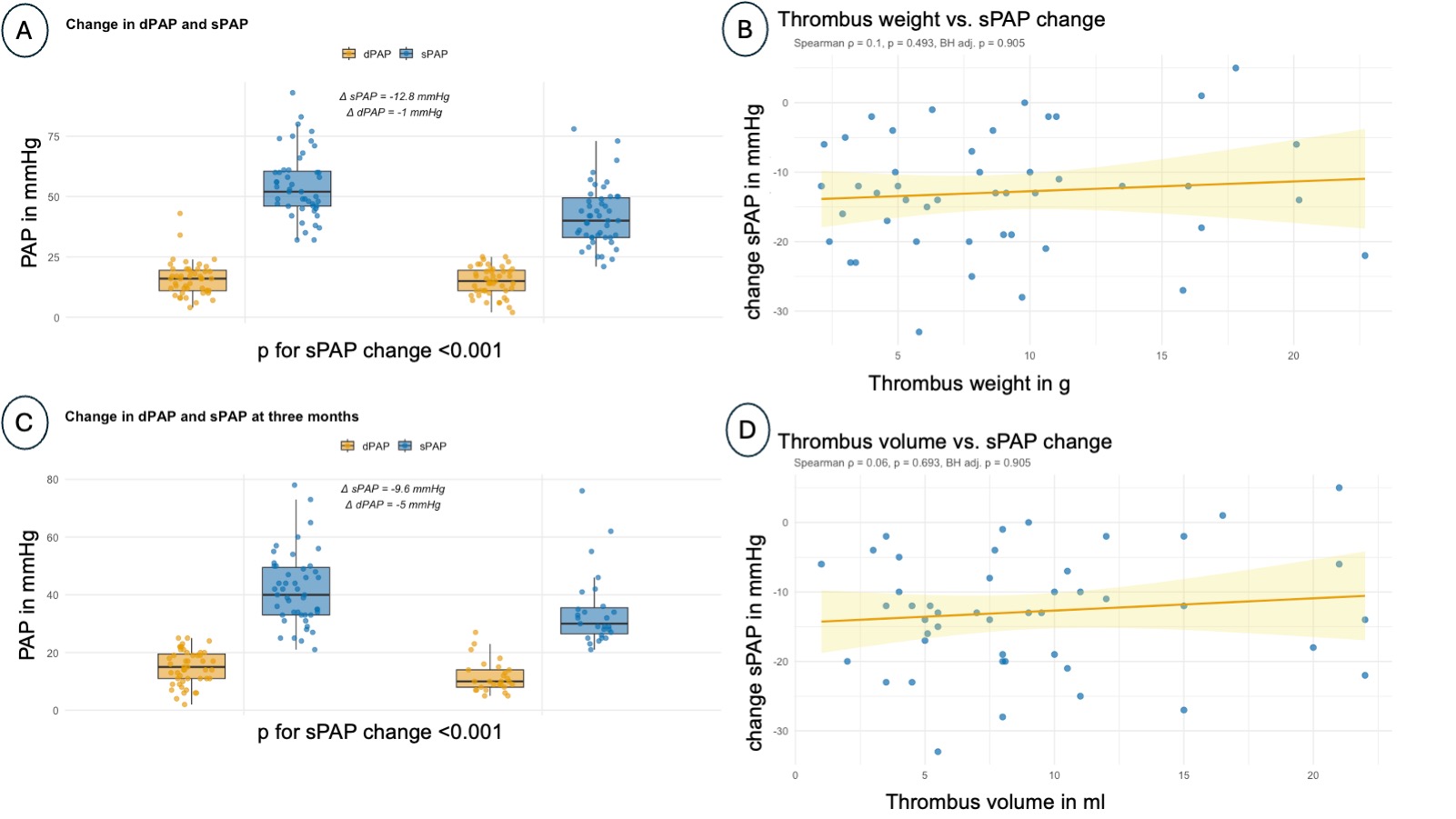
Data on thrombus mass and volume were available for 48 patients, all of whom had invasive follow-up at 3 months. A total of 41 patients were classified as intermediate-high risk and 7 patients as high-risk PE. Median thrombus mass was 7.8 (interquartile range (IQR) 4.8–10.6 g), median thrombus volume 8.0 ml (IQR 5.0-11.0 ml). Large-bore thrombectomy led to a reduction in systolic pulmonary artery pressures measured on table (-12.8 mmHg, p<0.001), a significant increase of right ventricular (RV) uncoupling from baseline to discharge (+0.235, p<0.01), and a significant decrease in the RV to left ventricular ratio (RV/LV-ratio) (-0.28, p<0.01). Right ventricular end diastolic diameter (RVEDD) as measured by echocardiography decreased from baseline to discharge (-8 mm, p<0.01), as did NT-proBNP (-2455 ng/l, p<0.001), and high-sensitivity cardiac Troponin T (hs-cTnT) (-48 ng/l, p<0.01).
Aspirated thrombus weight did not correlate with changes in on-table sPAP (Spearman r=0.1, p=0.49, adjusted p=0.90), change in RV-uncoupling from baseline to discharge (r=0.46, p=0.03, adjusted p=0.3), or change in RV/LV-ratio from baseline to discharge (r=-0.1, p=0.56, adjusted p=0.91). Similarly, no correlations were observed between thrombus weight and changes in RVEDD (r=0.09, p=0.61, adjusted p=0.91), hs-TnT (r=-0.08, p=0.62, adjusted p=0.91), or nt-proBNP (r=-0.04, p=0.81, adjusted p=0.97) from baseline to discharge. At three months, aspirated thrombus weight was also not correlated with changes in sPAP (r=0.35, p=0.07, adjusted p=0.35).
Conclusions
Thrombus weight and volume were not associated with postprocedural changes in invasive hemodynamics, RV function, or biomarkers of cardiac strain following large-bore thrombectomy for acute PE.