Background
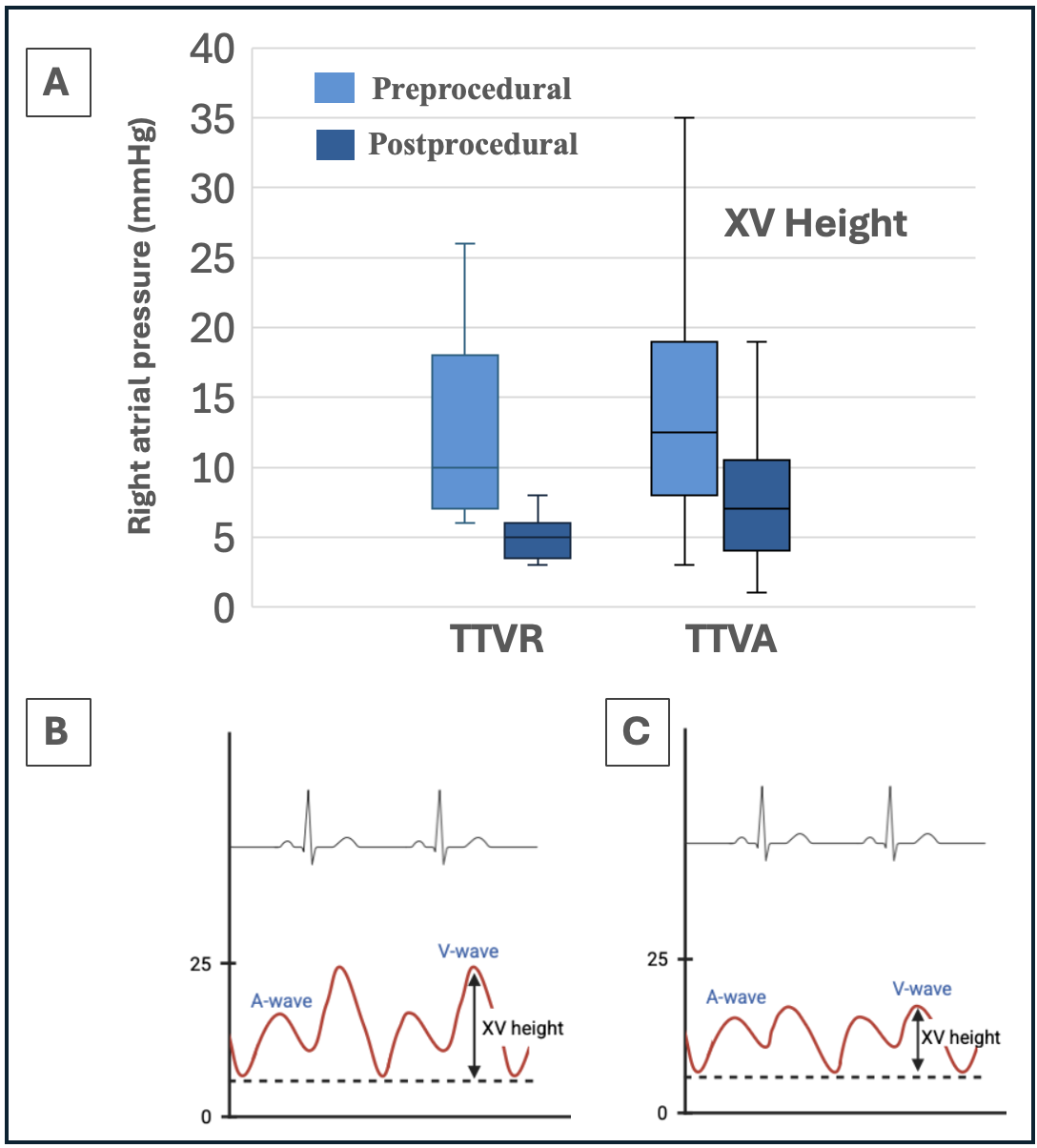
Transcatheter tricuspid valve replacement (TTVR) with the Evoque system offers effective elimination of tricuspid regurgitation (TR) in high-risk patients. Hemodynamics play a crucial role in this population, as elevated right atrial pressure (RAP) pre- and postprocedurally has been associated with worse outcomes in patients undergoing transcatheter tricuspid valve annuloplasty (TTVA) and edge-to-edge repair. This observation is particularly evident through XV height, defined as the difference between the V-wave and the nadir of RAP.
Methods
Patients with symptomatic severe functional TR who underwent TTVR in 2022 – 2025 were retrospectively analyzed. Invasive right heart catheterization was performed to measure right ventricular (RV) and atrial pressures before and after implantation. Data were compared to a cohort of patients who underwent TTVA between 2019 and 2022. The primary endpoint was defined as the postprocedural change in XV height (mmHg).
Results
13 patients undergoing TTVR and 58 undergoing TTVA with complete right atrial hemodynamic assessment were included. All patients presented with torrential (41%), massive (38%), or severe (21%) TR. Median age was 80 (75 – 83) years. Intraprocedural success according to TVARC criteria was achieved in all TTVR cases and in 58.6% of TTVA cases, with a residual TR grade of <II in 100% and 63.8% of cases, respectively. Postprocedural residual TR was reduced to grade I or less in all TTVR cases.
Hemodynamic assessment in TTVR and TTVA showed comparable preprocedural RAP values in both groups (XV height 12 mmHg [8 – 19]; p=0.36). RAP (mean/V-wave) decreased significantly postprocedural, with the most pronounced change observed in XV height (12 to 6 mmHg [4 – 10]; p<0.001). Postprocedural XV height in the TTVR group was 5 mmHg (3.5 – 6) compared to 7 mmHg (4 – 10.5) in the TTVA group, showing significantly lower RAP after Evoque implantation (p=0.043).
Overall systolic RV pressure increased from 42 mmHg (37 – 49) to 50 mmHg (45 – 58) postprocedurally (p<0.001), with a numerically greater postprocedural increase in the TTVR group (10 mmHg [+9]) compared with the TTVA group (5 mmHg [+9]; p=0.11).
Conclusions
TTVR with the Evoque system in patients with severe TR led to a reduction in RAP, particularly evident in the significantly lower XV height, and to a nominal increase in RV pressure. Despite the limited cohort size, the findings suggest a more pronounced hemodynamic effect of TTVR compared with TTVA. Larger patient cohorts and long-term follow-up studies are warranted to confirm these observations and to establish potential associations between hemodynamic improvements and clinical outcomes.