Background
“Jena auf Ziel” (“JaZ”) is a prospective cohort study in patients with ST-elevation myocardial infarction (STEMI). Early combination of a Atorvastatin 80mg and Ezetimibe 10mg was initiated on the day of admission and lipid-lowering therapy (LLT) was escalated during follow-up with bempedoic acid (BA) and PCSK9 inhibitors (PCSK9-I) to reach guideline-recommended LDL-cholesterol (LDL-C) levels. During the initial follow-up period of 12 months, all patients reached the recommended ESC/EAS LDL-C target for very high-risk patients of <55mg/dL.
Methods
After 12 months, patients could either continue regular follow-up in the specialized outpatient lipid clinic or transition to standard care with their general practitioners (GPs). 36.5% of patients remained in the lipid clinic, and 63.5% chose GP-based follow-up. Differences in LDL-C levels, therapy adherence, and major adverse cardiovascular events (MACE = nonfatal ischemic events, heart failure hospitalization, or nonfatal stroke) were analyzed over a 48-month follow-up.
Results
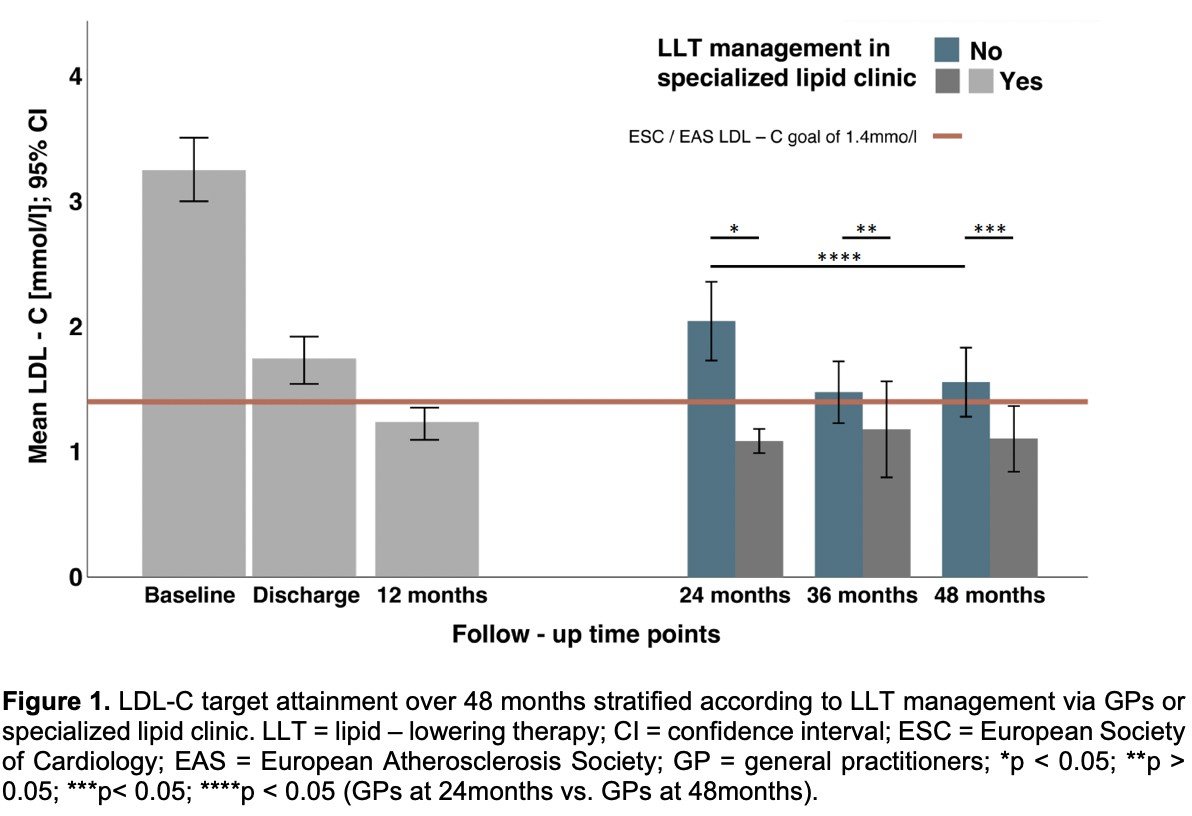
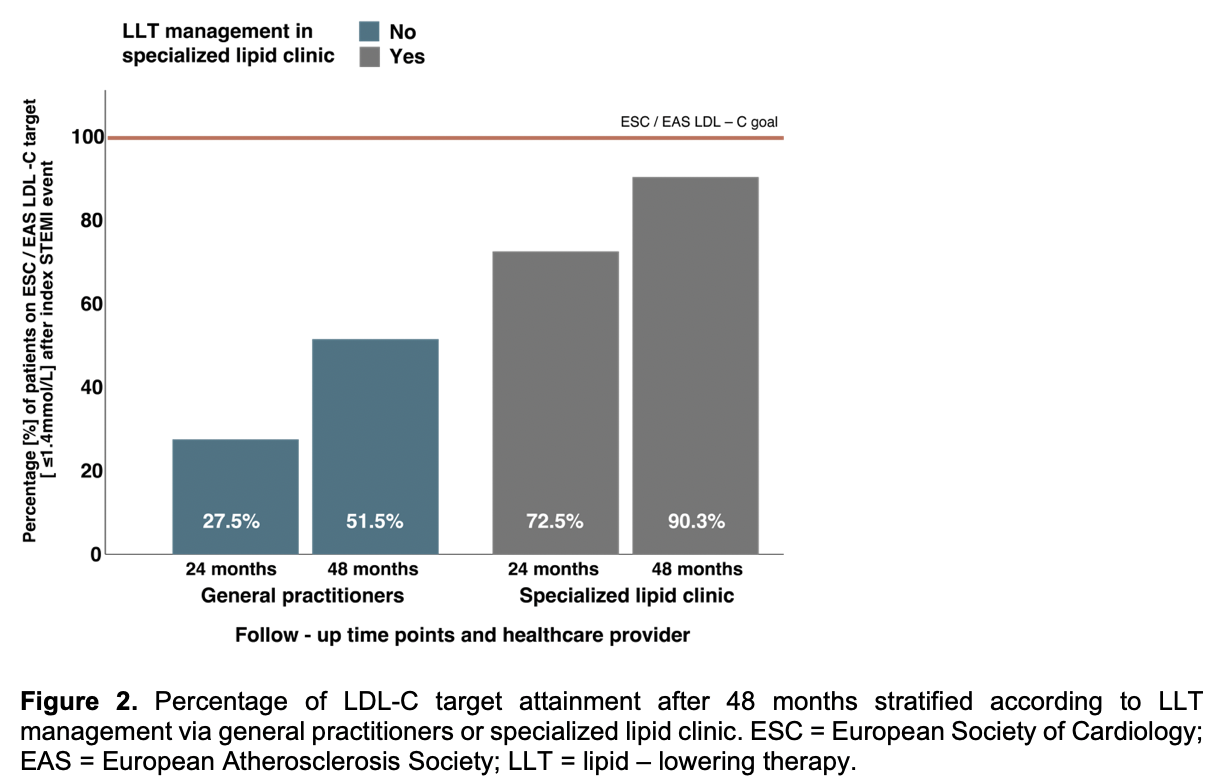
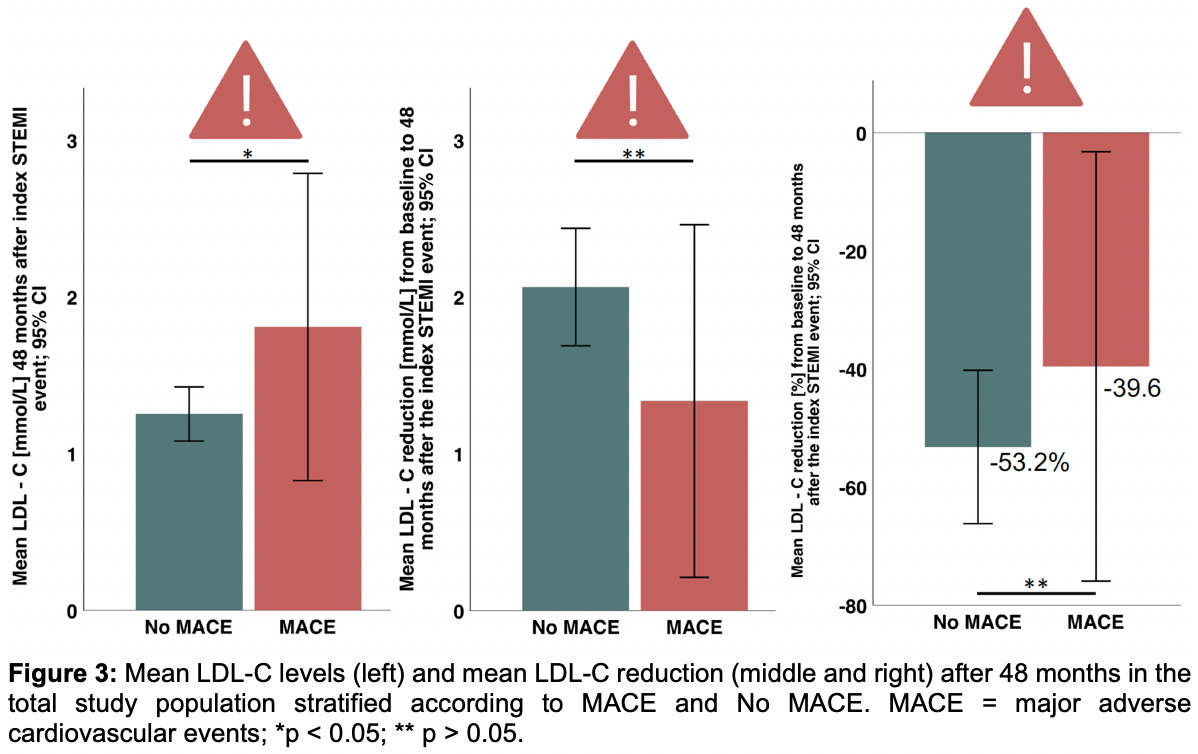
Initially, a total of 85 consecutive patients were included in this study at the index event. 73 (85.9%) were male, 12 (14.1%) were female, the average age was 64.4±13.1 years. All 85 patients were followed for 4 years. During the 48-month follow-up, 10 patients died, and 14 experienced a MACE. Mean LDL-C level in the total study population at 48 months was 1.34±0.81 mmol/L and 70.3% were on target. Patients treated by GPs had higher LDL-C levels compared to those followed in the lipid clinic (1.56±0.77mmol/L vs. 1.10±0.77mmol/L; p = 0.024; Figure 1). However, GP-managed patients showed significant improvement in LDL-C reduction over time, from 2.10±0.79mmol/L at 24 months to 1.55±0.77mmol/L at 48 months (p = 0.0086); Figure 1. LDL-C target attainment increased from 24 to 48 months in both groups (Figure 2): from 72.5% to 90.3% among patients in the specialized lipid clinic and from 27.5% to 51.5% among GP-treated patients. Despite this improvement, MACE patients still exhibited significantly higher LDL-C levels than non-MACE patients (1.81±1.40mmol/L vs. 1.25±0.63 mmol/L; p = 0.04), Figure 3. The mean LDL-C reduction from baseline to 48 months was 2.06±1.37 mmol/L (-53.2±47.11%) in the non-MACE group and 1.33±1.57mmol/L (-39.6±50.8%) in the MACE group, although this difference was not statistically significant (p = 0.069), Figure 3. The distribution of MACE at 48 months was independent of the type of follow-up care (GP: 9 patients [17.0%] vs. lipid clinic: 5 patients [16.1%]; p = 0.59).
Conclusion
The 4 -year follow-up of the “Jena auf Ziel” cohort reveals, that LDL-C management in primary care improved significantly over time, narrowing the treatment gap compared to specialized lipid clinics. Nevertheless, specialized lipid clinic follow-up remained superior in maintaining LDL-C targets. Persistent differences in LDL-C control highlight the importance of structured lipid management and long-term follow-up in high-risk cardiovascular patients.