Background: Frailty is a key predictor of outcomes in older patients with heart failure (HF), yet it is rarely assessed systematically in clinical practice. The electronic Frailty Index () enables automated frailty detection from health records through the assessment of a multi-dimensional item-set of frailty-associated comorbidities, symptoms, disabilities and abnormal test results, but its validity and prognostic value in acute HF (AHF) remain uncertain. This study aimed to (1) determine frailty prevalence, (2) describe patient characteristics across the ejection fraction (EF) spectrum, and (3) examine its association with all-cause death and HF rehospitalization in patients with AHF.
Methods: Data from the prospective CYCLE cohort were retrospectively analyzed, including patients hospitalized with and with complete data for eFI calculation; follow-up continued through July 2024. The eFI was calculated by dividing the number of deficits present by the total number of available deficits, yielding a value between 0 and 1. Frailty as assessed by the eFI was subsequently categorized as mild (0.13-0.24), moderate (0.25-0.36), or severe (>0.36). Associations between frailty status and outcomes were analyzed using and Kaplan-Meier methods adjusted for age, male sex and lactate levels at baseline.
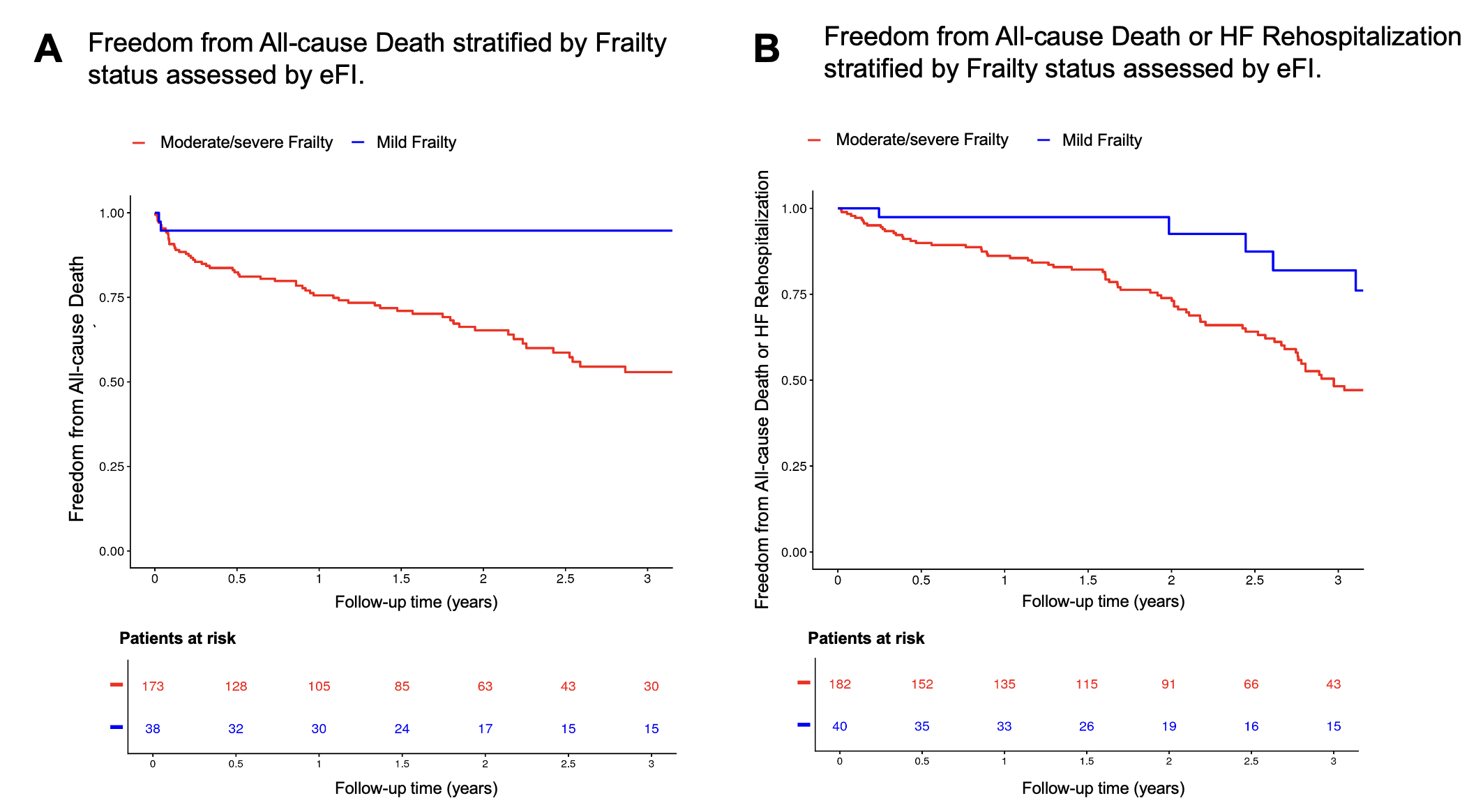
Results: Among 222 patients hospitalized with AHF (71 years old (interquartile range 61-80), 157 men (70.7%)), 18.0% had mild, 41.9% moderate, and 40.1% severe frailty. The median age increased with frailty severity (57 years in mild, 71 years in moderate, and 75 years in severe frailty; p<0.001). Most patients were male (70.7%). Increasing frailty status was associated with a higher prevalence of comorbidities, including hypertension (45.0%, 65.6%, and 80.9%; p<0.001), diabetes (7.5%, 30.1%, and 38.6%; p=0.0016), chronic kidney disease (7.5%, 24.2%, and 55.7%; p<0.001), coronary artery disease (7.5%, 45.7%, and 64.0%; p<0.001), and atrial fibrillation (28.2%, 52.7%, and 66.3%; pHigher frailty status was also associated with higher NT-proBNP and hs-CRP, lower hemoglobin and cystatin C-based estimated glomerular filtration rate, and higher NYHA class. During a median of 2.08 [IQR 1.88; 2.57] years, 68 deaths occurred. Compared with severe frailty, mild frailty was associated with a lower risk of all-cause death (HR 0.18, 95% CI 0.05-0.47; p<0.001) as well -0.63, p<0.001) (Figure 1A and B) after adjustment for age, male sex and lactate levels at baseline.
Conclusion: In this contemporary cohort of patients with AHF, higher frailty was associated with higher risk of all-cause death and the composite of all-cause death or HF rehospitalization. These hypothesis-generating findings support the use of the eFI to identify high-risk AHF
Key Words: acute heart failure; frailty; electronic frailty index; mortality; outcomes.