Background
In patients with mechanical aortic and mitral valves, catheter ablation(CA) of ventricular tachycardia(VT) is challenging, as conventional left ventricular(LV) access is impossible. We report a unique case of right atrium-to-left ventricle(RA-to-LV) access for VT ablation guided by CT imaging merged with a 3D mapping system.
Case Presentation
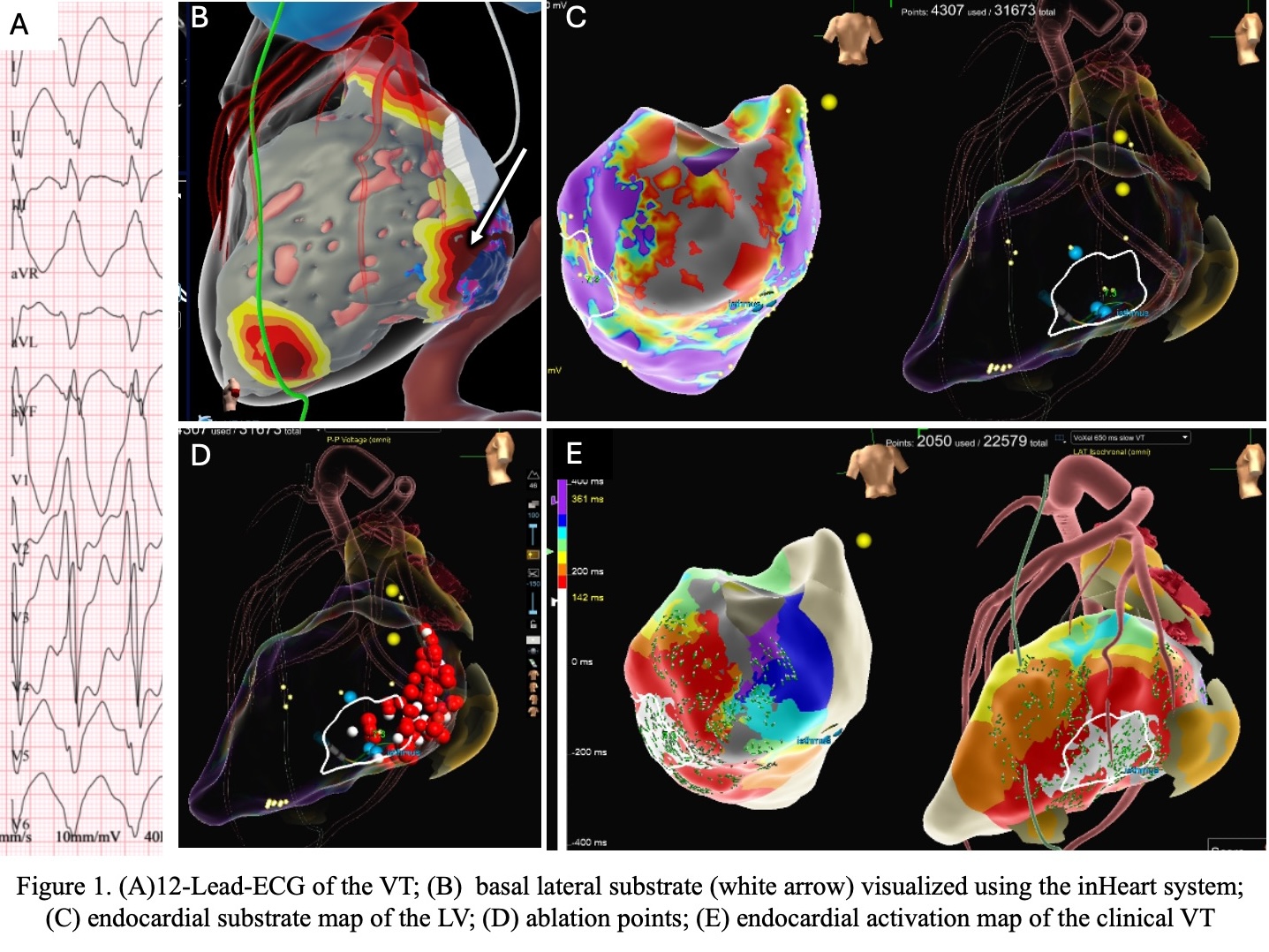
A 60-year-old woman with dilated cardiomyopathy, two mechanical valves, and LVEF(15%) was admitted with VT storm. She had previously undergone stereotactic and alcohol ablation of a basal inferolateral LV substrate(Fig.1A). Despite antiarrhythmic therapy(propranolol, amiodarone, mexiletine), VT recurred. ICD interrogation showed >3,700 slow VT episodes terminated by antitachycardia pacing over two months. The 12-lead ECG revealed slow VT(110 bpm) with morphology consistent with a basal lateral exit(Fig.1B). As no further therapy escalation was possible and thoracotomy or transapical access were refused, an RA-to-LV approach was chosen as a bailout strategy.
The procedure was performed under general anesthesia. Three femoral venous accesses were obtained. Intracardiac echocardiography(ICE) was unavailable, and transesophageal echocardiography(TEE) guidance was limited. A 3D reconstruction of the RA and tricuspid valve region was performed using the EnSiteX system with a magnetically navigated catheter and merged with a CT-based 3D model of the RA and LV(inHeart system). The optimal puncture site for RA-to-LV access was tagged and marked fluoroscopically.
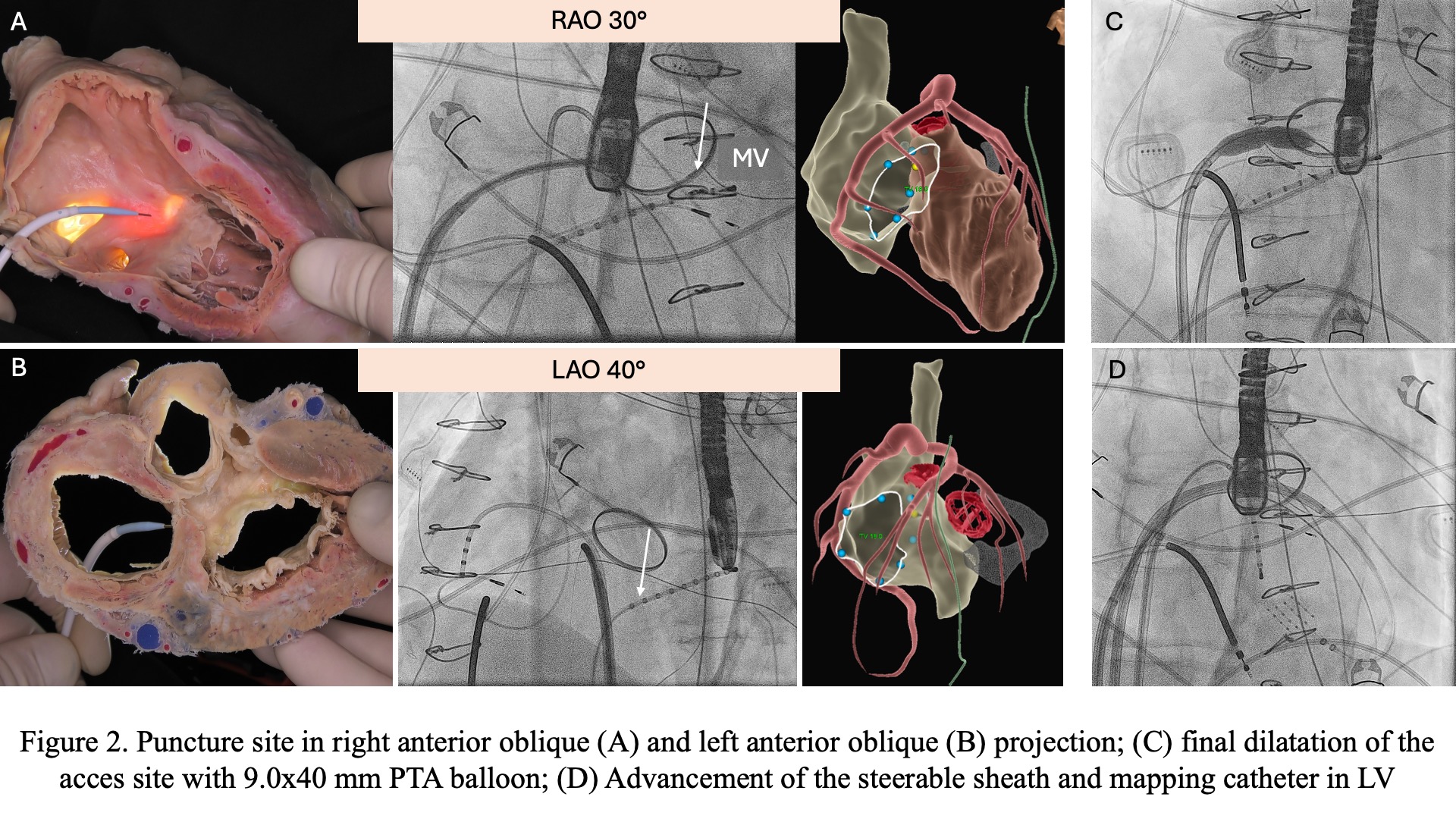
Direct puncture of the inferior-medial RA wall was performed using a steerable sheath and a long transseptal needle(98 cm, BRK-1) guided by fluoroscopic marks(Fig.2A,B). To overcome tissue rigidity, short RF delivery was applied at the needle tip. After advancing the needle and guidewire into the LV, the puncture site was dilated using various balloons, including cutting and PTA 9.0×40 mm(Fig.2C), allowing sheath and mapping catheter advancement(Fig.2D).
Substrate mapping revealed a low-voltage area on the basal inferior wall(Fig.1C). Activation mapping showed a reentrant circuit with the VT isthmus in the basal posterolateral LV(Fig.1D). RF ablation(50 W) at this site terminated VT and rendered it non-inducible. After sheath removal, TEE and right heart catheterization confirmed no LV-to-RA shunt. No complications occurred. The patient was discharged in stable condition and remained free of sustained VT at short-term follow-up.
Conclusion
RA-to-LV access may represent a feasible and safe option for VT ablation in patients with “no-entry” LV and can be performed using CT imaging merged with a 3D mapping system even when echocardiographic guidance is unavailable or limited.