Case Presentation:A patient was admitted to our clinic for evaluation of severe anemia after having received six red blood cell transfusions at an external hospital. Gastrointestinal bleeding was excluded by gastroscopy and colonoscopy. On admission, hemoglobin was 5.1 g/dL, creatinine 3.3 mg/dL, and pro-BNP markedly elevated at 9890 ng/L (reference ≤879 ng/L). To investigate the elevated pro-BNP, an echocardiogram was performed.
Cardiac Diagnostics:Echocardiography showes a mildly enlarged left ventricle with severely reduced systolic function. A mobile, wall-adherent structure was identified in the apical and midventricular region of the left ventricle, resembling a “Batman signal” (Fig. 1a).
Cardiac magnetic resonance imaging (MRI) confirmed a severely reduced left ventricular ejection fraction of 30% with an end-diastolic diameter of 69 mm and an end-diastolic volume index of 96 mL/m² (Fig. 1b, 1d). The right ventricle showed an end-diastolic volume index of 120 mL/m² (upper limit of normal) and an ejection fraction of 42% (Fig. 1c). No myocardial edema was present. The apical structure in the left ventricle demonstrated no contrast enhancement, consistent with a thrombus. Late gadolinium enhancement revealed patchy intramural fibrosis in the basal and septal ventricular segments (Fig. 1f). Increased trabeculation of the left ventricle suggested a non-dilated left ventricular cardiomyopathy. Thickening of the basal posterior mitral leaflet (Fig. 1b) was consistent with non-bacterial thrombotic endocarditis. The “Batman signal” structure likely represented a thrombus arising from the trabeculated myocardium.
Non-Cardiac Diagnostics:MRI also revealed a mass lesion located anterior to the ascending aorta and posterior to the sternum. Histopathological evaluation confirmed a thymoma, WHO type A, associated with pure red cell aplasia (bone marrow erythropoietic hypoplasia/aplasia, paraneoplastic). Thoracic CT demonstrated mediastinal lymph nodes suspicious for metastases. Cranial CT revealed multiple post-ischemic lesions in the posterior circulation.
During hospitalization, the patient developed progressive heart failure with multiorgan failure and subsequently passed away.
Discussion:This case illustrates the interplay between a paraneoplastic thymoma, hematologic and thrombotic complications, and cardiomyopathy. The coexistence of biventricular dysfunction with late gadolinium enhancement supported the diagnosis of non-dilated cardiomyopathy. The thymoma-induced pure red cell aplasia likely contributed to a prothrombotic state, leading to non-bacterial thrombotic endocarditis and the formation of a left ventricular thrombus, which produced a “Batman signal” appearance. Comprehensive non-cardiac evaluation is crucial in similar cases to identify systemic or paraneoplastic causes underlying complex cardiac findings.
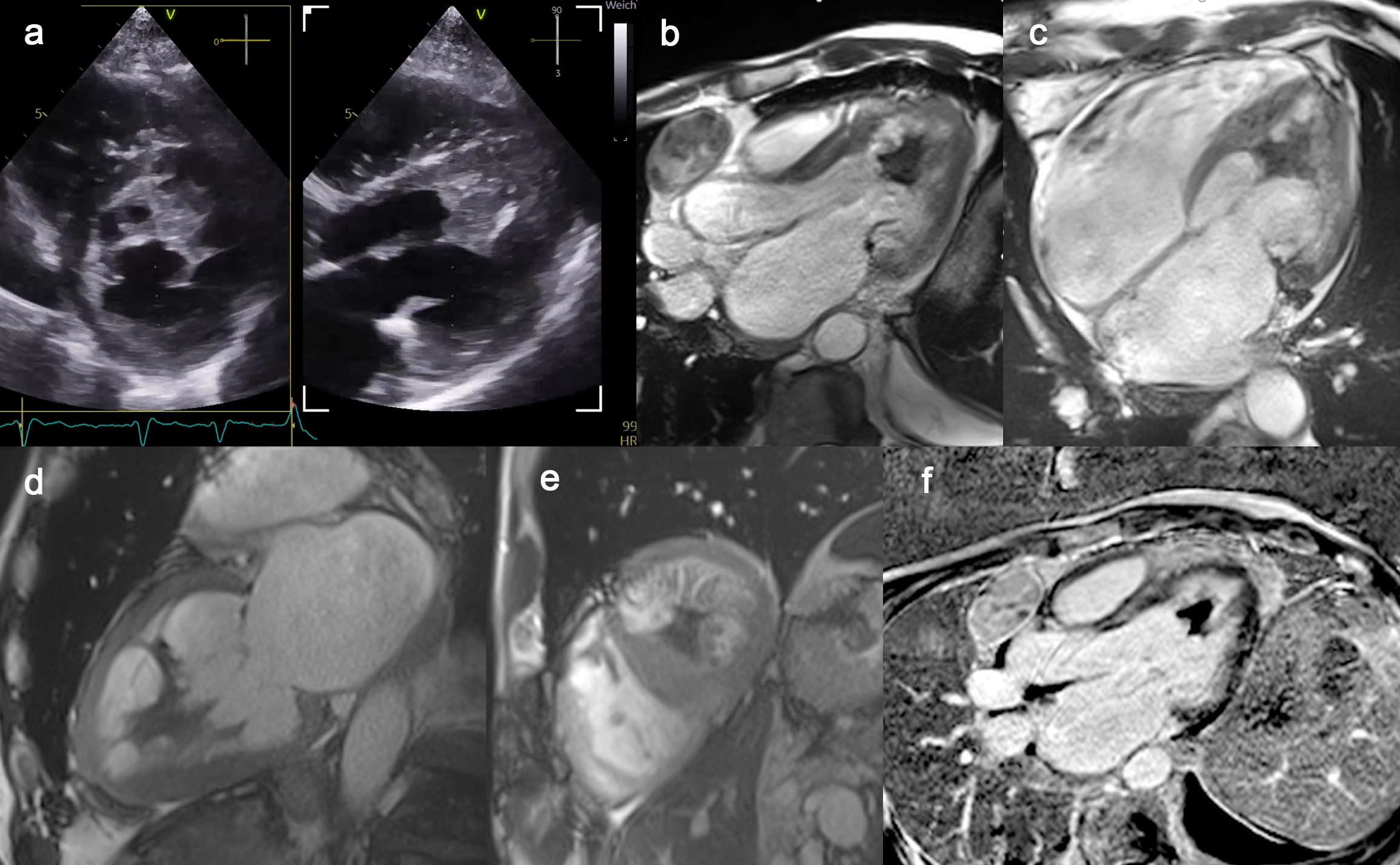
Figure 1: Echocardiography and magnetic resonance imaging of a non-dilated cardiomyopathy, non-bacterial thrombotic endocarditis and a left ventricular thrombus appearing as a “Batman signal” in the left ventricle



