Introduction
Papillary fibroelastoma (PFE) is a rare cardiac tumor, occurring in about 0.038% of patients undergoing echocardiography. Although often asymptomatic, it carries a high risk of embolic events.
Case presentation
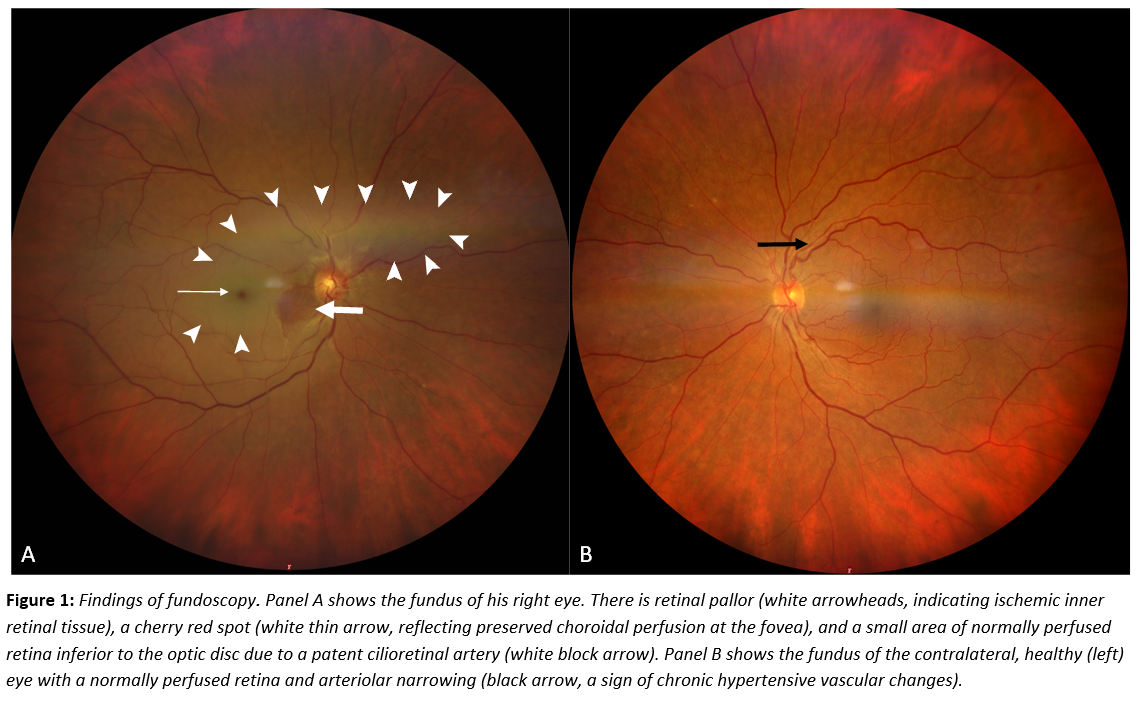
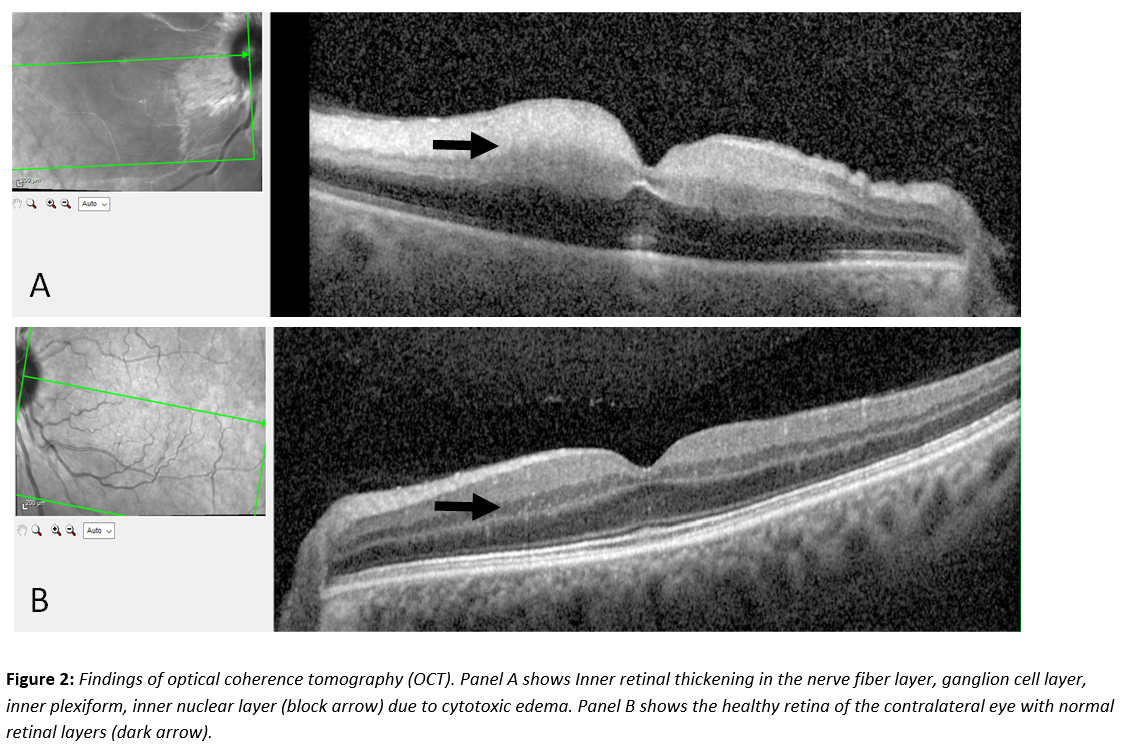
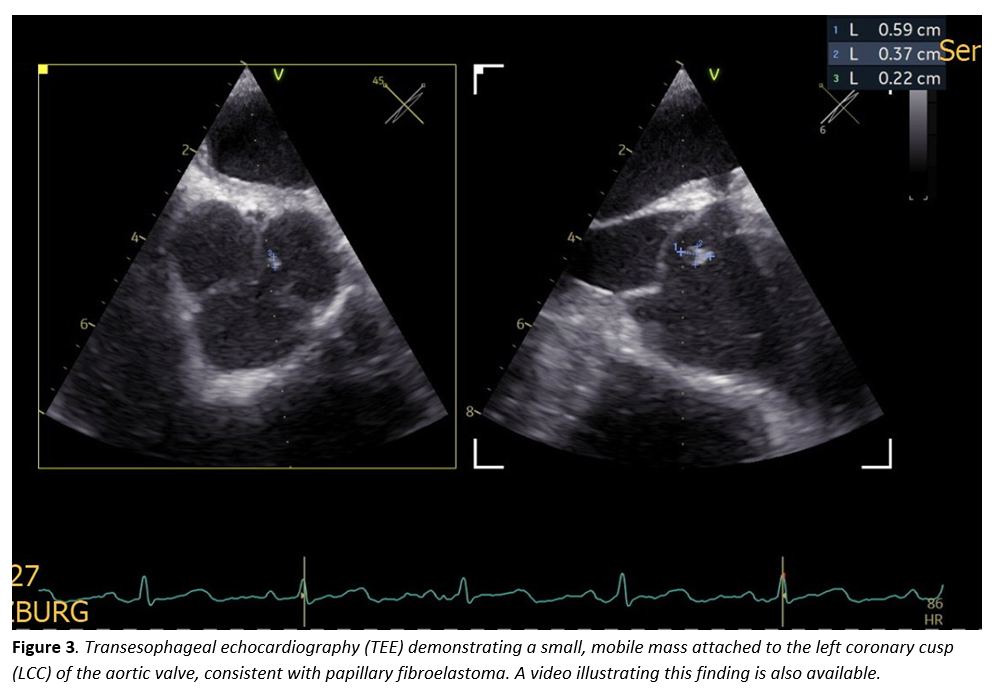
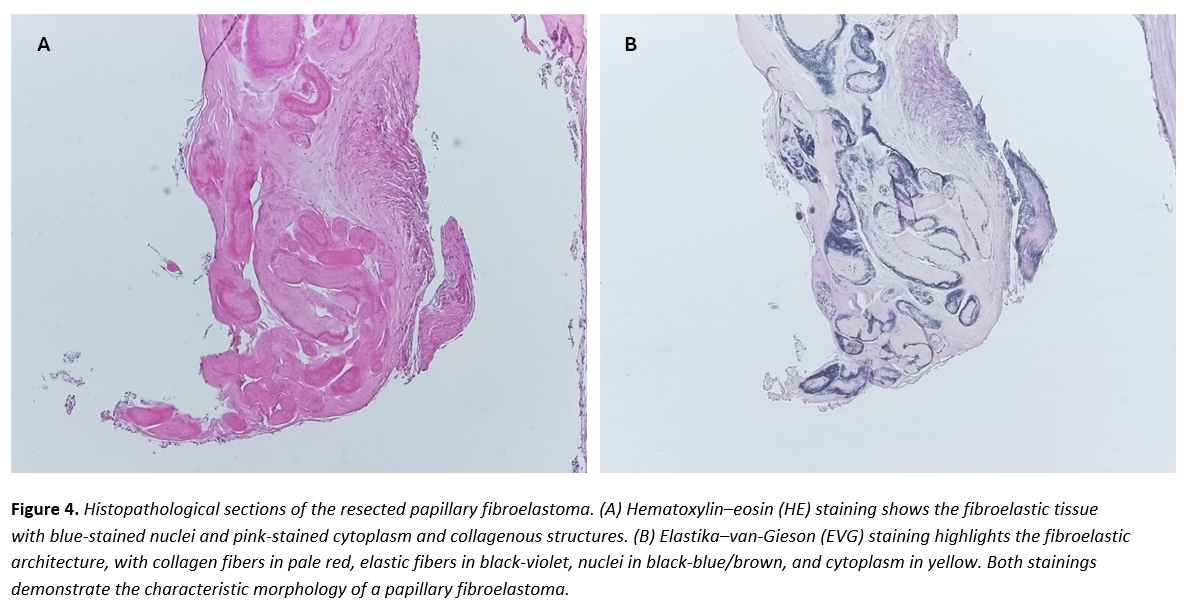
A 61-year-old woman with arterial hypertension presented with acute, painless vision loss in the right eye. Ophthalmologic examination confirmed central retinal artery occlusion (Figures 1–2). Routine laboratory tests, including inflammatory markers and coagulation profile, were normal. ECG and 24-hour monitoring showed sinus rhythm, and carotid Doppler sonography excluded relevant stenosis. Transesophageal echocardiography revealed a small, mobile mass attached to the left coronary cusp of the aortic valve (Figure 3). The lesion was faintly visible on transthoracic echocardiography but not detected by CT. After coronary CT excluded significant stenosis, surgical resection under cardiopulmonary bypass was performed. The tumor was completely excised with valve preservation. Histopathology confirmed PFE (Figure 4). The postoperative course was uneventful; however, severe vision loss in the right eye persisted, consistent with irreversible central retinal artery occlusion.
Discussion
PFE, though histologically benign, is clinically relevant due to its embolic potential. In a systematic review of 161 patients, ischemic stroke occurred in 68% and transient ischemic attack in 32%, while visual symptoms appeared in 17%. Isolated central retinal artery occlusion as an initial sign is exceedingly rare. Even very small tumors can cause devastating ischemia, as shown in this case, emphasizing the importance of early detection. Diagnosis relies on imaging, with transesophageal echocardiography being the most sensitive tool for identifying small, mobile lesions, while CT or transthoracic echocardiography may miss them. Although no formal international guidelines exist, surgical excision is strongly recommended for symptomatic left-sided fibroelastomas due to their high embolic risk. In most cases, valve-sparing shave resection is sufficient, and recurrence after surgery is rare. This case illustrates that central retinal artery occlusion, though uncommon, can be the first manifestation of PFE. Early recognition and surgical treatment may prevent further embolic events.
Conclusion
We report a rare case of PFE presenting as isolated central retinal artery occlusion. Cardiac tumors should be considered in the differential diagnosis of ocular embolism, and transesophageal echocardiography is essential for detection. Surgical excision remains the treatment of choice to prevent recurrent embolic events.