Background and Aims: The use of iodinated contrast agents during cardiovascular procedures carries the risk of kidney injury. Although contrast-induced nephropathy is well recognized in the acute setting, the potential impact of contrast volume on medium- to long-term renal function remains unclear. This study aimed to assess the association between cumulative contrast volume and subsequent medium- to long-term changes in renal function in patients with repeated percutaneous coronary interventions (PCI).
Methods: This retrospective single-center study included all patients who underwent repeated PCIs between 2003 and 2023, with intervals of ≥7 days and ≤365 days between procedures. Volume of contrast agent administered during the initial intervention as well as estimated glomerular filtration rate (eGFR) values at the time of the initial PCI and at readmission were extracted from hospital records. Renal function was classified using the “Kidney Disease: Improving Global Outcomes” (KDIGO) staging system. The primary endpoint was progression to a higher KDIGO stage at readmission, excluding patients initially at stage G5, as further deterioration was not possible. Secondary endpoint was association with eGFR, analyzed in relation to the contrast volume and potential confounders.
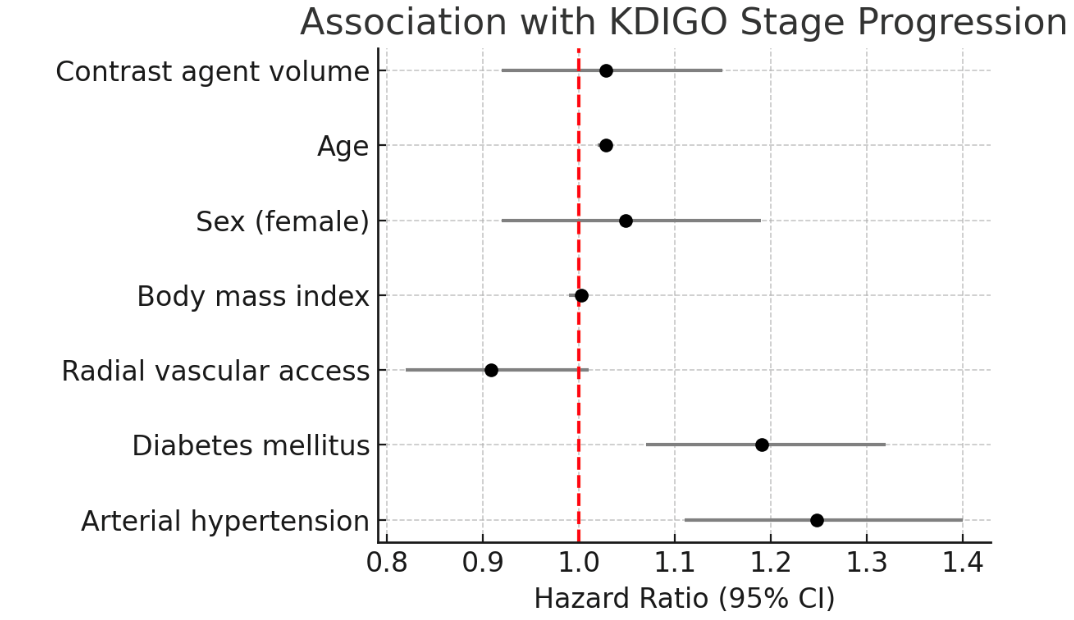
Results: A total of 6,714 patients were included in the study. The mean age was 67.2 ± 10.4; 80.2% were male. KDIGO stage analysis was available for 6,611 patients. Baseline mean eGFR was 74.4 ± 21.5 mL/min/1.73 m². The median interval between procedures was 127 days. The median contrast volume administered was 220 mL. At readmission, mean eGFR was 72.2 ± 21.6 mL/min/1.73 m². 1,700 patients (25.7%) had KDIGO stage progression. In univariable analyses, contrast volume was not significantly associated with KDIGO stage progression (HR: 1.08; 95% CI: 0.98-1.19) or reduced eGFR (Estimate: 0.31, 95% CI: -0.64-1.25). Multivariable analyses confirmed these findings. In contrast, diabetes mellitus (KDIGO: HR: 1.19; 95% CI: 1.07-1.32, eGFR: Estimate -3.17; 95% CI: -4.15- -2.18), arterial hypertension (KDIGO: HR: 1.25; 95% CI: 1.11-1.40, eGFR: Estimate -2.92; 95% CI: -3.94- -1.89), and age (KDIGO: HR: 1.03; 95% CI: 1.02-1.03, eGFR: Estimate -0.13; 95% CI: -0.18- -0.08) were significantly associated with worse renal outcomes.
Conclusion: No association was observed between the cumulative contrast volume administered during PCI and medium- to long-term deterioration of renal function in patients undergoing repeated procedures. Instead, diabetes mellitus, arterial hypertension, and age emerged as the main predictors of renal impairment at readmission.