Background and Aims: Contrast-induced nephropathy remains a challenge in cardiovascular procedures. Since contrast volume and the vascular access route are considered key modifiable risk factors, volume minimization and the use of a transradial access have become cornerstones of preventive strategies. While earlier recommendations proposed fixed contrast thresholds, contemporary approaches emphasize individualized assessment, such as the maximum allowable contrast dose (MACD), which accounts for body weight and baseline renal function. MACD exceedance and a transfemoral access have been linked to higher risks of acute kidney injury. However, whether this also contributes to medium- to long-term renal decline remains unclear. Therefore, we aimed to investigate this association in patients undergoing repeated percutaneous coronary interventions (PCI).
Methods: In this subgroup analysis of a retrospective single-center study, patients with repeated PCI between 2003 and 2023 with an interval of ≥7 and ≤365 days between procedures were included. The MACD was calculated for each patient according to the original formula (5×body weight [kg]/serum creatinine [mg/dL], maximum dose 300 mL). Renal function was classified according to the Kidney Disease: Improving Global Outcomes (KDIGO) staging system. The primary endpoint was the risk of KDIGO stage progression at readmission. Secondary endpoints were associations with eGFR.
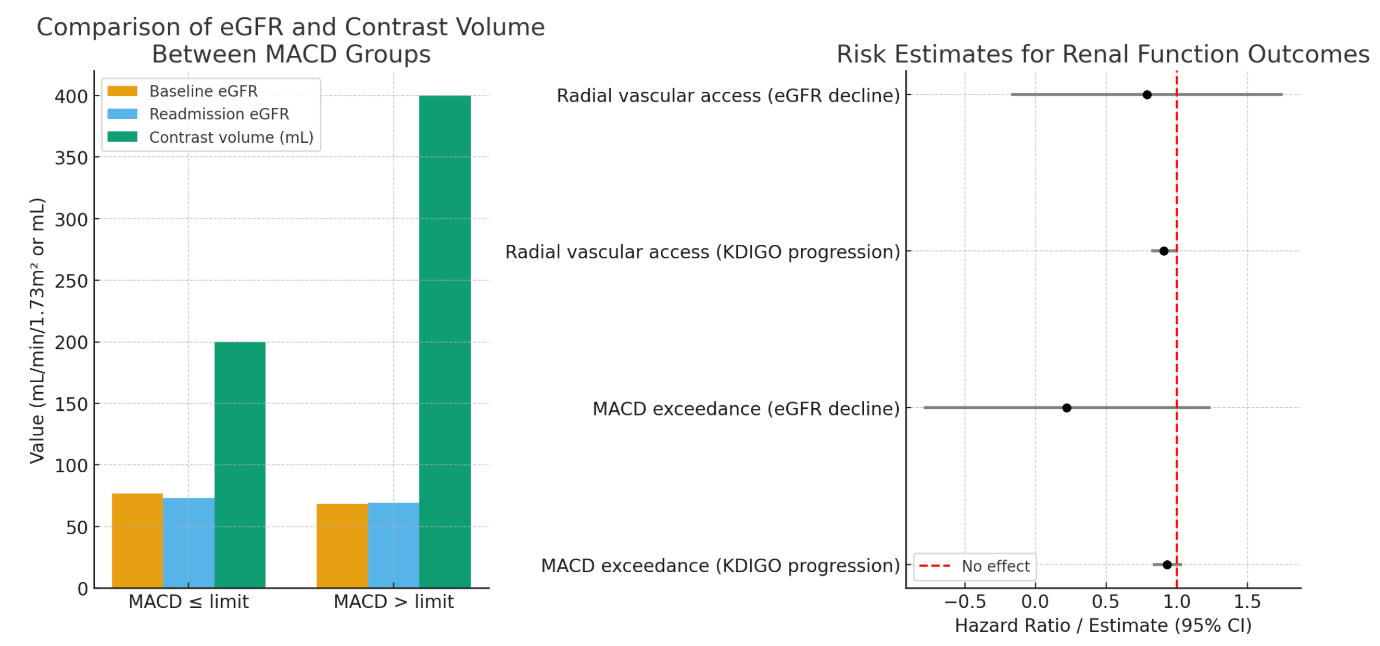
Results: In 1,814 (27%) of the 6,714 patients included in the study, the contrast volume administered during the index PCI exceeded the MACD. The median MACD was 300 mL in both groups. The median contrast volume administered was substantially higher in the exceedance group (400 mL vs. 200 mL). These patients had lower mean eGFR (68.5 ± 26.1 vs. 76.6 ± 19.0 mL/min/1.73 m²) at baseline. Other baseline characteristics were similar between groups. At readmission, mean eGFR was 69.25 ± 24.3 mL/min/1.73 m² in the exceedance group (vs. 73.24 ± 20.4 mL/min/1.73 m² in non-exceedance group). Univariable analyses showed no significant association between MACD exceedance and increased risk of KDIGO progression (HR 0.93; 95% CI: 0.83-1.04) or eGFR (Estimate: 0.22; 95% CI: -0.79-1.24) at follow-up, which was confirmed in multivariable analyses.
In 2,500 patients (37.2%) the initial PCI was performed via radial access. Despite a trend towards lower risk for renal impairment at readmission, ultimately no statistically significant association was found (KDIGO: HR 0.91; 95% CI: 0.82-1.01; eGFR: Estimate 0.79; 95% CI: -0.17-1.75).
Conclusion: Neither the chosen vascular access route nor exceeding the individual MACD during PCI were associated with a decline in medium- to long-term renal function in patients with repeated interventions within one year.