Background:
Left bundle branch area pacing with a single defibrillator lead (LBBAD) has recently emerged as a novel therapeutic option for patients requiring both implantable cardioverter-defibrillator (ICD) implantation and cardiac resynchronization therapy (CRT). Evidence on its acute and mid-term performance remains limited.
Methods:
Patients with a primary or secondary preventive ICD indication and additional CRT indication were included in a retrospective single-center registry. A DF-4 ICD lead was implanted with the aim of left bundle branch pacing, and defibrillation testing was performed in all procedures. Procedural success and safety were assessed, and short-term follow-up was conducted at 30 days and mid-term follow-up at ≥60 days. Device- and ECG-related, echocardiographic, and clinical parameters were compared with baseline.
Results:
Seventeen patients (median age 70 [interquartile range 56; 76] years, 88% male; 65% with primary preventive ICD indication) were included. Heart failure was present in 15/17 (88%) patients, with ischemic (n=6), pacemaker-aggravated (n=4), or non-ischemic etiologies (n=5), and 14 patients had a left ventricular ejection fraction (LVEF) ≤35%. High-grade atrioventricular block was present in 59% and sick sinus syndrome in 6% of patients.
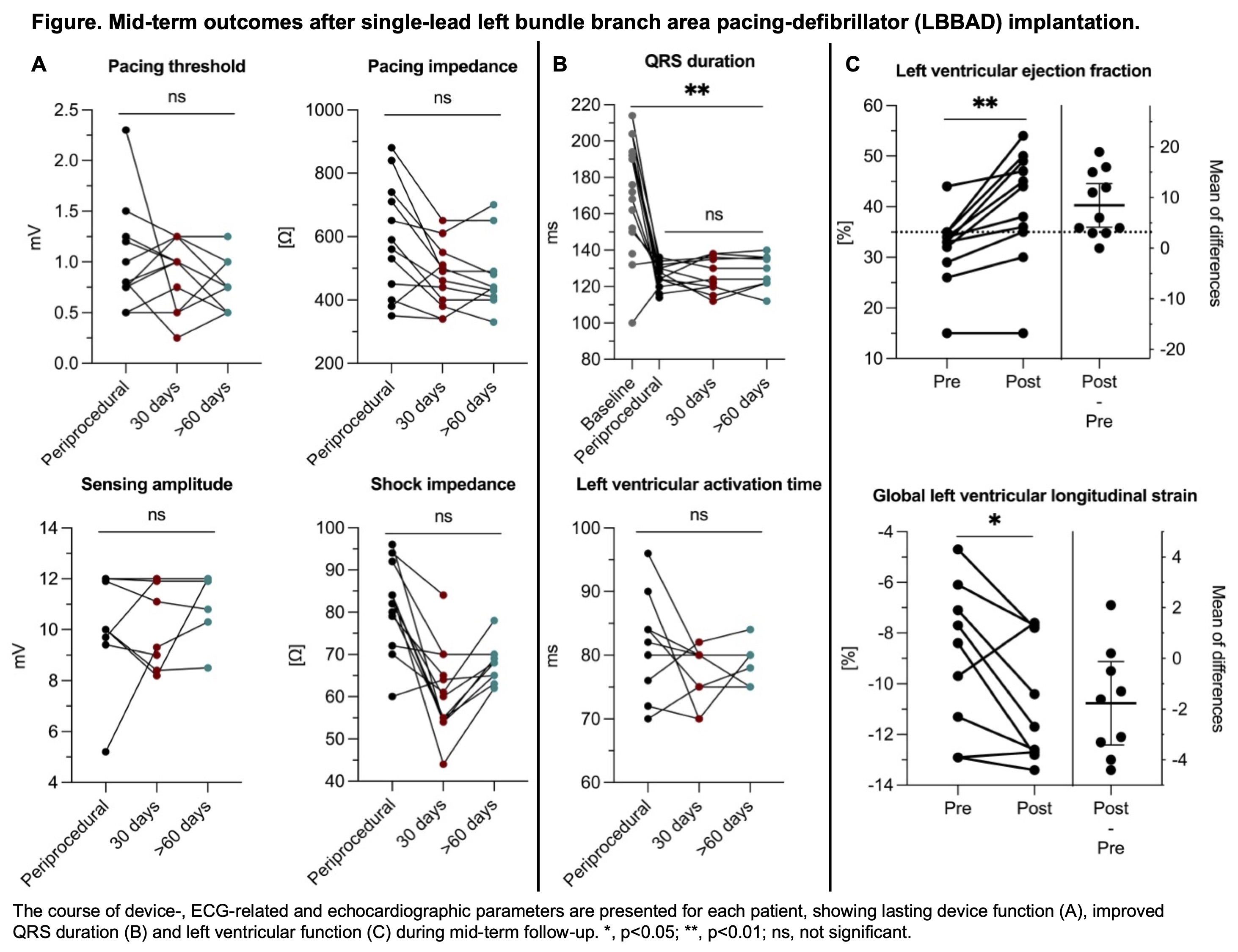
LBBAD implantation was successful in 14/17 patients (82%) (median procedure duration 120 minutes, fluoroscopy time 11 minutes, 2 [1; 3] screw-in attempts). Effective defibrillation was confirmed in all tested patients. Two patients required left bundle branch pacing-optimized-CRT due to persistent QRS prolongation. Acute pacing parameters were within normal limits (median pacing threshold 0.8 mV, sensing 11.9 mV, pacing impedance 545 Ω, shock impedance 83 Ω). QRS duration decreased from 172 [150; 193] ms to 128 [122; 133] ms (p<0.001). Median left ventricular activation time and V6–V1 inter-peak interval were 81 [76; 84] ms and 54 [44; 60] ms. Implantation failed in three patients due to no possible left bundle branch capture or sensing loss. No periprocedural complications occurred.
Short-term follow-up was available in 13 patients and mid-term follow-up in 10 patients (median 240 [104; 358] days). Device- and ECG-related parameters remained stable (Figure A and B). Median LVEF increased from 33 [27; 35] % to 44 [35; 49] % (p=0.001), with 7/9 (78%) primary-prevention patients improving from ≤35% to >35% (Figure C). Median left ventricular end-diastolic volume (161 [139; 188] ml to 129 [107; 160] ml, p=0.020) and global longitudinal strain (–8.4 [-12.1; -6.6] % to –11.7 [-12.8; -7.8] %, p=0.034) improved significantly. One patient experienced an appropriate ICD shock for ventricular fibrillation 14 days post-implantation and one an inappropriate shock due to permanent AF with rapid ventricular response.
Conclusion:
Single-lead LBBAD implantation is safe, feasible, and provides durable pacing and defibrillator performance. Mid-term follow-up demonstrated significant QRS narrowing and improved left ventricular function with reverse remodeling. Given the high rate of LVEF recovery in primary-prevention patients, further studies are warranted to refine ICD indication in this population.