Background
The diagnosis and treatment of heart failure with preserved ejection fraction (HFpEF) remain highly challenging, in part because the condition is often recognized only at advanced stages, when structural remodelling has occurred or patients already present with symptoms. Identifying early markers of impending diastolic dysfunction (DD) in at-risk individuals is therefore crucial to enable targeted preventive strategies. Given the pivotal role of left atrial (LA) function in the pathophysiology of DD and HFpEF, this study aimed to evaluate its potential to identify patients at increased risk of progressive diastolic impairment.
Methods
We prospectively recruited 99 patients at risk for HFpEF who were referred for consultations unrelated to heart failre between 02–11/2024. Inclusion required ≥1 HFpEF risk factor (age>60y, hypertension, diabetes, chronic kidney disease, or obesity). Patients with manifest HFpEF or LVEF<50% were excluded; all were in sinus rhythm at baseline. Each participant underwent baseline and 12-month follow-up assessments including transthoracic echocardiography. LA function (morphology and speckle-tracking strain) was analyzed blinded to outcomes. The primary endpoint was DD progression, defined as a ≥1-point increase in the HFA-PEFF score after one year. Groups were compared using the Mann–Whitney U and χ²-test. The predictive performance of different parameters was evaluated by receiver operating characteristic (ROC) analysis and compared using the area under the curve (AUC).
Results
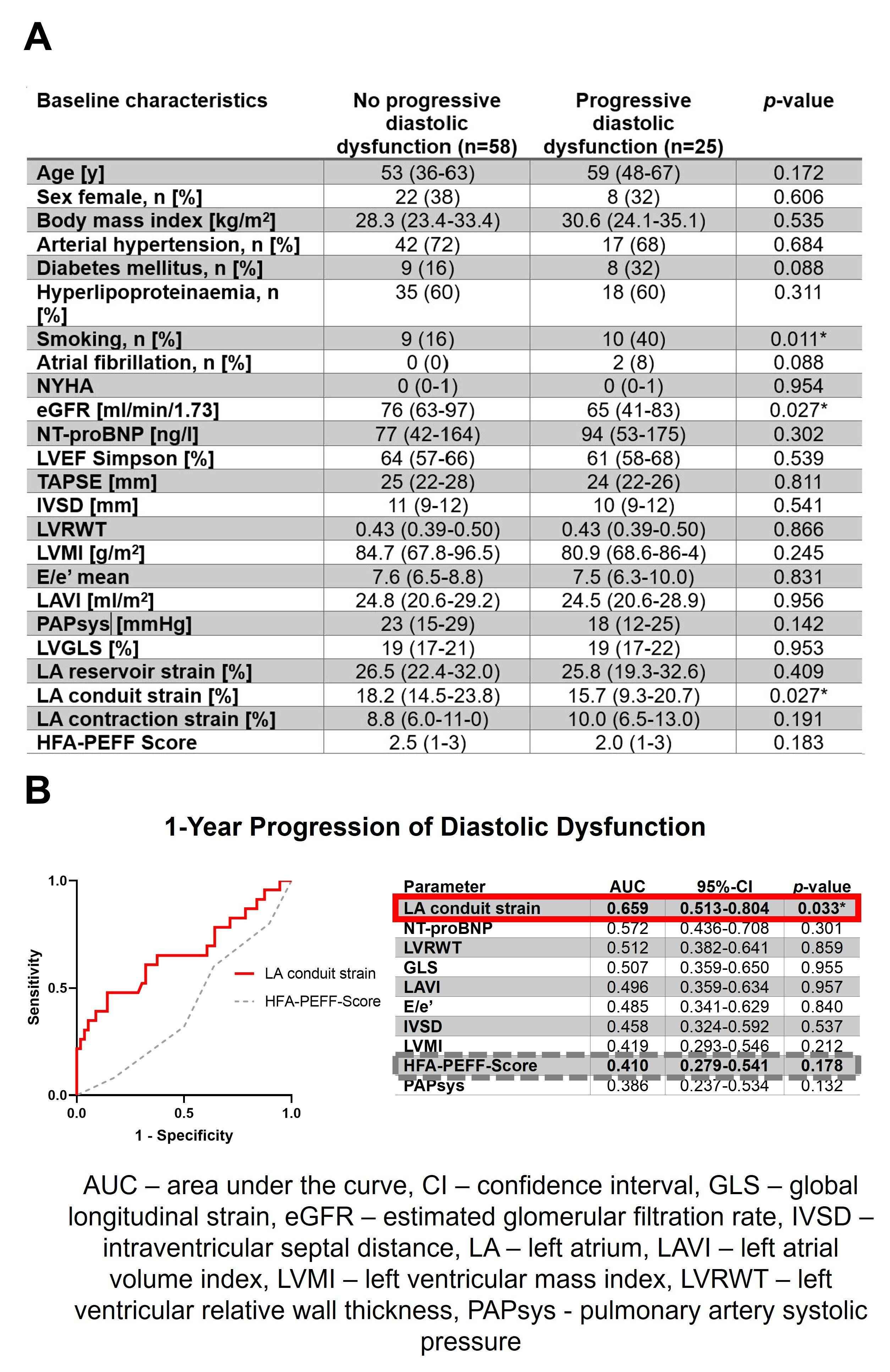
Following the exclusion of 13 patients who were newly diagnosed with HFpEF at baseline and 3 patients with an LVEF <50%, the final cohort comprised 83 patients (30 [36%] female; aged 53±17 years). Over a mean follow-up of 13.0±1.4 months, 25 patients (30%) experienced progression of DD, including five patients (6%) developing manifest HFpEF. Patients with progressive DD were of comparable age and sex distributions compared to those without, while they had worse renal function (estimated glomerular filtration rates: p=0.027) (Figure 1A). There was no difference in median HFA-PEFF scores at baseline in both groups (2.0 [1-3] vs. 2.5 [1-3], p=0.183). However, patients with progressive DD had a lower LA conduit strain compared to those without progression (15.7% [9.3-20.7] vs. 18.2% [14.5-23.8], p= 0.027), while other ventricular, atrial and functional markers of diastolic function were comparable across both groups. ROC analysis showed that LA conduit strain had the highest AUC to predict future progression of DD (0.659 [0.513-0.804], p=0.033) outperforming other individual markers of diastolic function and baseline HFA-PEFF score (0.410 [0.279-0.541], p=0.178) (Figure 1B).
Conclusion
Among at-risk individuals, impaired LA conduit strain emerged as an early marker of future progressive diastolic dysfunction, outperforming conventional parameters included in the HFA-PEFF score. Comprehensive assessment of LA function may enhance early identification of individuals at risk for developing diastolic heart failure.