Background
Atrial fibrillation (AF) is the most common arrhythmia in clinical practice. Multiple prior endocardial and epicardial ablations may create a highly complex atrial substrate and arrhythmogenic mechanisms, making subsequent touch-up ablations particularly challenging.
Case report
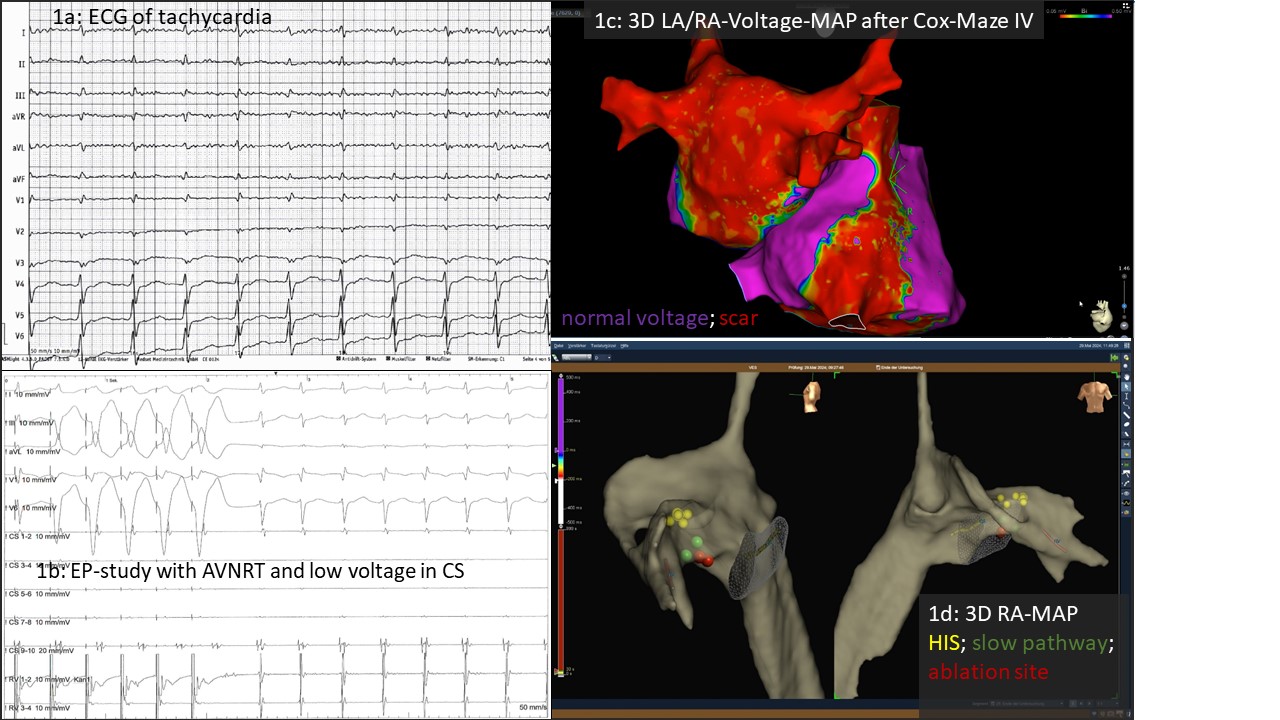
We present a 63-year-old, athletically active patient with a five-year history of highly symptomatic AF. Since 2019, he underwent six left atrial (LA) endocardial ablation procedures in high-volume centers, including pulmonary vein (PV) isolation and extensive substrate modification (three with radiofrequency, three with pulsed field ablation). During the sixth procedure, durable isolation of all PVs, a complete LA posterior box, and cavotricuspid isthmus (CTI) block were confirmed. In December 2023, a surgical biatrial Cryo Cox-Maze IV procedure was subsequently performed at our center. Following surgery, the patient still complained of exercise-induced palpitations lasting several hours (ECG Fig. 1a) and presented for touch-up ablation.
EP study
Voltage mapping after Cox-Maze IV confirmed durable PV isolation, an intact posterior LA box, complete CTI block, and a cavo-caval right atrial line (Fig. 1c). Surprisingly, programmed atrial stimulation induced typical AV nodal reentrant tachycardia (AVNRT) rather than the expected LA tachycardia (Fig. 1b). The patient identified this arrhythmia as clinically relevant. Following successful slow pathway modification (Fig. 1d), the patient continues to be free of arrhythmia.
Discussion
Management of persistent LA tachyarrhythmias after multiple ablations is complex. Surgical biatrial ablation may represent a valuable option in experienced centers. This case highlights that the endocardial created tricuspid line as well as the surgical leasion up to the right atrial appendage may alter the electrophysiology of Koch’s triangle, potentially facilitating AVNRT. Thus, precise knowledge of both, the surgical and catheter-based lesions is essential for electrophysiologists performing touch-up ablations, as atrial signals can be difficult to interpret after extensive biatrial procedures. Moreover, even when only AF or LA tachycardia is suspected, programmed atrial stimulation at the beginning of the procedure may uncover alternative arrhythmia mechanisms.