Background:
Idiopathic outflow tract premature ventricular contractions (PVCs) are most commonly localized in the right ventricular outflow tract (RVOT). The clinical significance of sustained outflow tract ventricular tachycardia (OT-VT) regarding any predominance to one specific anatomic area remains uncertain.
Subjective:
This study aimed to characterize the clinical and procedural features of patients with idiopathic sustained OT-VT and determine whether the site of origin can be predicted from clinical presentation.
Methods:
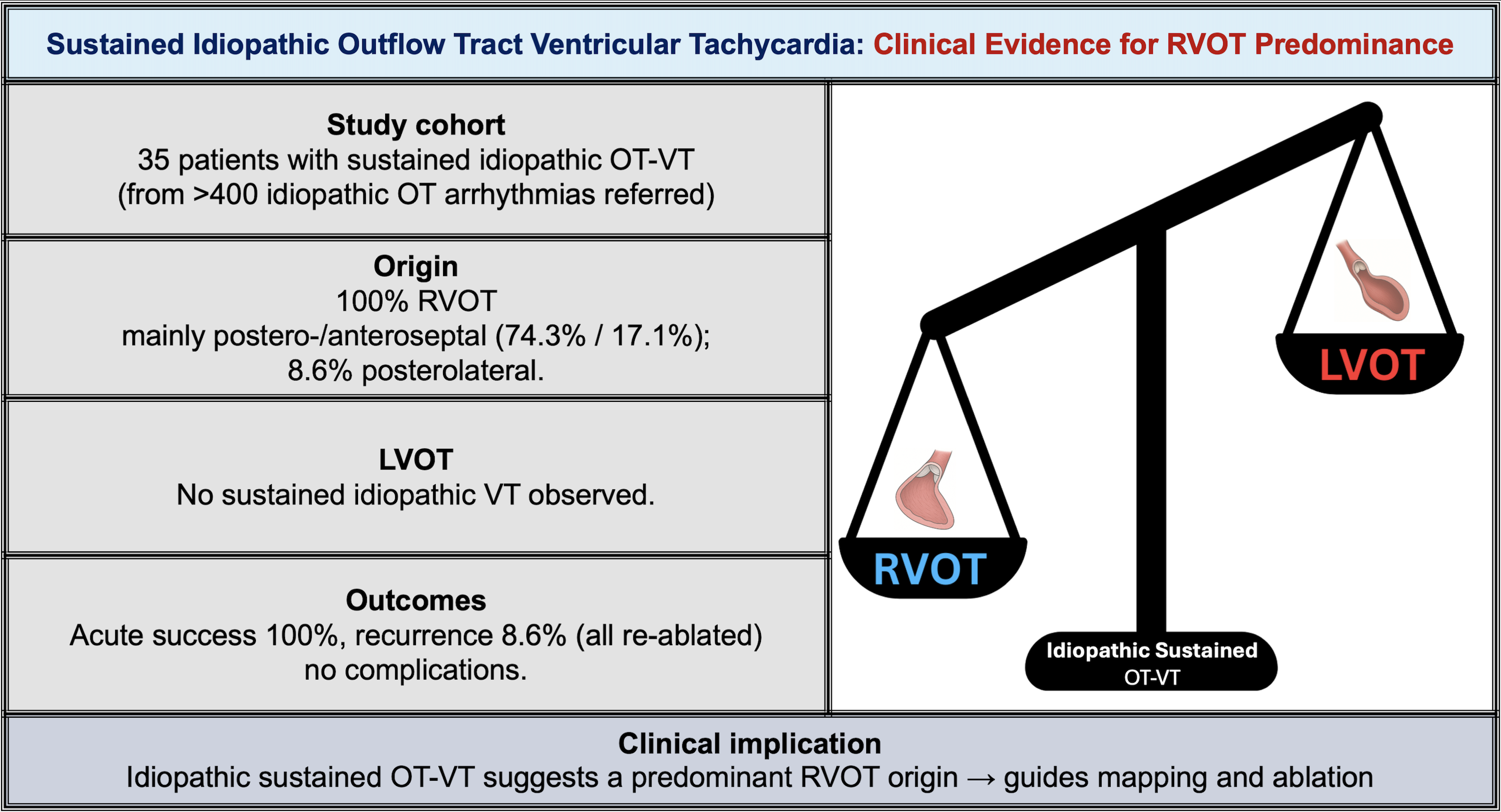
This retrospective cohort included 35 consecutive patients with documented sustained OT-VT (≥30 seconds), from over 400 patients referred for idiopathic outflow tract arrhythmia ablation. Baseline clinical and echocardiographic characteristics were collected and procedural data reviewed. Sites of arrhythmia origin were identified by electroanatomic mapping and ablation outcomes.
Results:
Sustained OT-VT arose exclusively from right-sided outflow tract foci, most commonly the postero- or anteroseptal RVOT (n=26, 74.3% and n=6, 17.1%, respectively) and less frequently from the posterolateral (n=3, 8.6%) (Figure 1). No cases of sustained VT from the LVOT were observed. Acute ablation success was achieved in all patients. During 12 months of follow-up, recurrence occurred in 3 patients (8.6%), all of whom were successfully managed with repeat ablation. No complications were observed.
Conclusion:
In patients with structurally normal hearts, sustained OT-VT in our cohort arose exclusively from the RVOT. Recognition of this pattern can guide mapping and ablation strategies.