Background:
Tricuspid regurgitation (TR) and right ventricular (RV) function are tightly interconnected. Determining optimal timing for intervention in patients with severe TR remains a major clinical challenge. The new ESC/EACTS valvular heart disease guidelines propose revised reference values for RV size and function, but these thresholds remain unvalidated and of uncertain predictive relevance.
Objectives:
To evaluate the predictive value of the guideline-recommended thresholds for RV size and function in patients undergoing transcatheter tricuspid valve repair (TTVr).
Methods:
We retrospectively analyzed high-surgical-risk patients who underwent tricuspid valve transcatheter edge-to-edge repair (T-TEER) or transcatheter tricuspid valve annuloplasty (TTVA) at a tertiary center in Germany. The primary endpoint was 2-year survival.
Results:
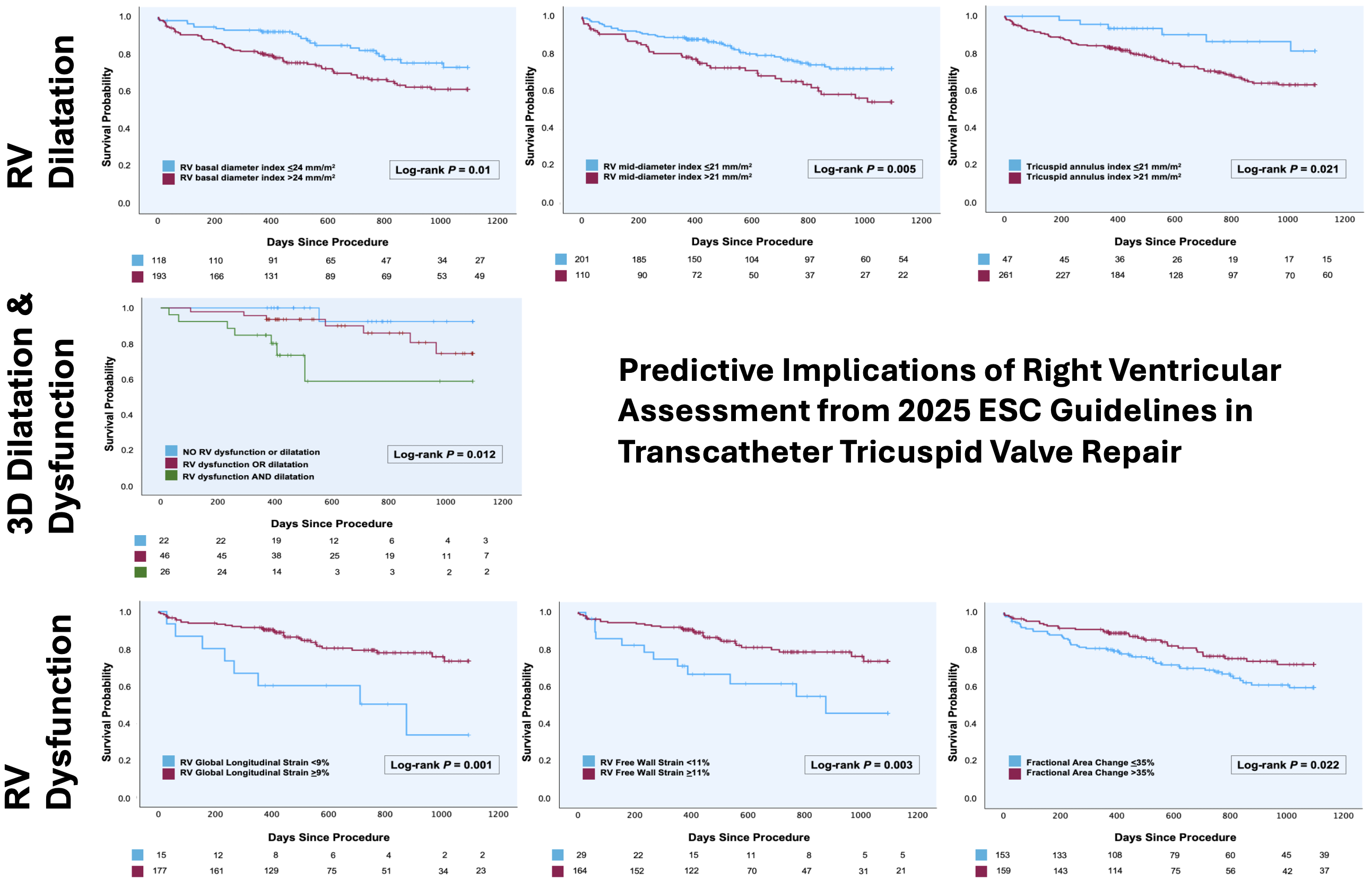
312 patients were included: 209 (67%) underwent T-TEER and 103 (33%) TTVA. The cohort was 68% female with a median age of 80 years (Q1-Q3: 76–83). Patients had severe (59%), massive (25%), or torrential TR (16%). Residual TR ≤II was achieved in 73% of procedures. Follow-up was 828 (726–930) days. For RV dilatation, proposed indexed cut-offs (RV basal >24 mm/m² and mid diameter >21 mm/m²) were associated with significant differences in 3-year survival (log-rank test: p=0.01; p=0.005, respectively). Nevertheless, the conventional non-indexed cut-off values (RV basal diameter >41 mm, RV mid diameter >35 mm) were also significant (p=0.048; p<0.001). A tricuspid annular diameter >21 mm/m² was associated with worse survival (p=0.021). In patients stratified by 3D volumes (n=94), RV end-diastolic volume index >95 ml/m² and RV end-systolic volume index >37 ml/m² were associated with worse survival (p=0.034; p=0.02). When applying RV dysfunction cut-offs, longitudinal parameters TAPSE (<17 mm) and RV TDI s’ (<10 cm/s) did not significantly discriminate between groups (p=0.21; p=0.052), whereas fractional area change <35% showed inferior survival (p=0.022).
Free wall strain <23% showed no significant association (p=0.095, n=192), whereas <11% indicating severe dysfunction was significant (p=0.003). Similarly, RV global longitudinal strain <21% was not significant (p=0.075), but <9% indicating severe dysfunction was highly significant (p=0.001).
The 3D RV ejection fraction <50% separated outcomes (p=0.041, n=94).
Stratification into groups by RV function and dilatation based on 3D parameters (none vs. dilatation or dysfunction vs. both) revealed the best survival in the first and the worst in the last group (p=0.012).
Conclusion:
TR intervention timing is crucial, as TTVr candidates are often referred late with advanced RV dysfunction and poor prognosis. Overall, proposed cut-offs from 2025 guidelines perform well and should guide risk stratification in clinical practice. In this real-world cohort, indexed RV basal and mid diameters were significantly associated with survival differences. Unidimensional parameters of RV function like TAPSE or TDI s′ fail to reflect the complex RV geometry and are insufficient for risk stratification alone. A multiparametric echocardiographic approach, including (indexed) 3D volumes, functional parameters, and RV strain showed better discrimination.