Background
Rare pathogenic variants that predispose to cardiomyopathy (CMP) increase the risk of adverse cardiovascular outcomes. However, their prevalence and prognostic relevance in contemporary cardiovascular (CV) trial populations are not well defined.
Objective
To determine the frequency of pathogenic or likely pathogenic (PLP) variants associated with dilated (DCM), hypertrophic (HCM), and arrhythmogenic right ventricular cardiomyopathy (ARVC) in large, well-characterized CV trial cohorts, and to evaluate their associations with prevalent heart failure (HF) and incident HF hospitalization (HHF).
Methods
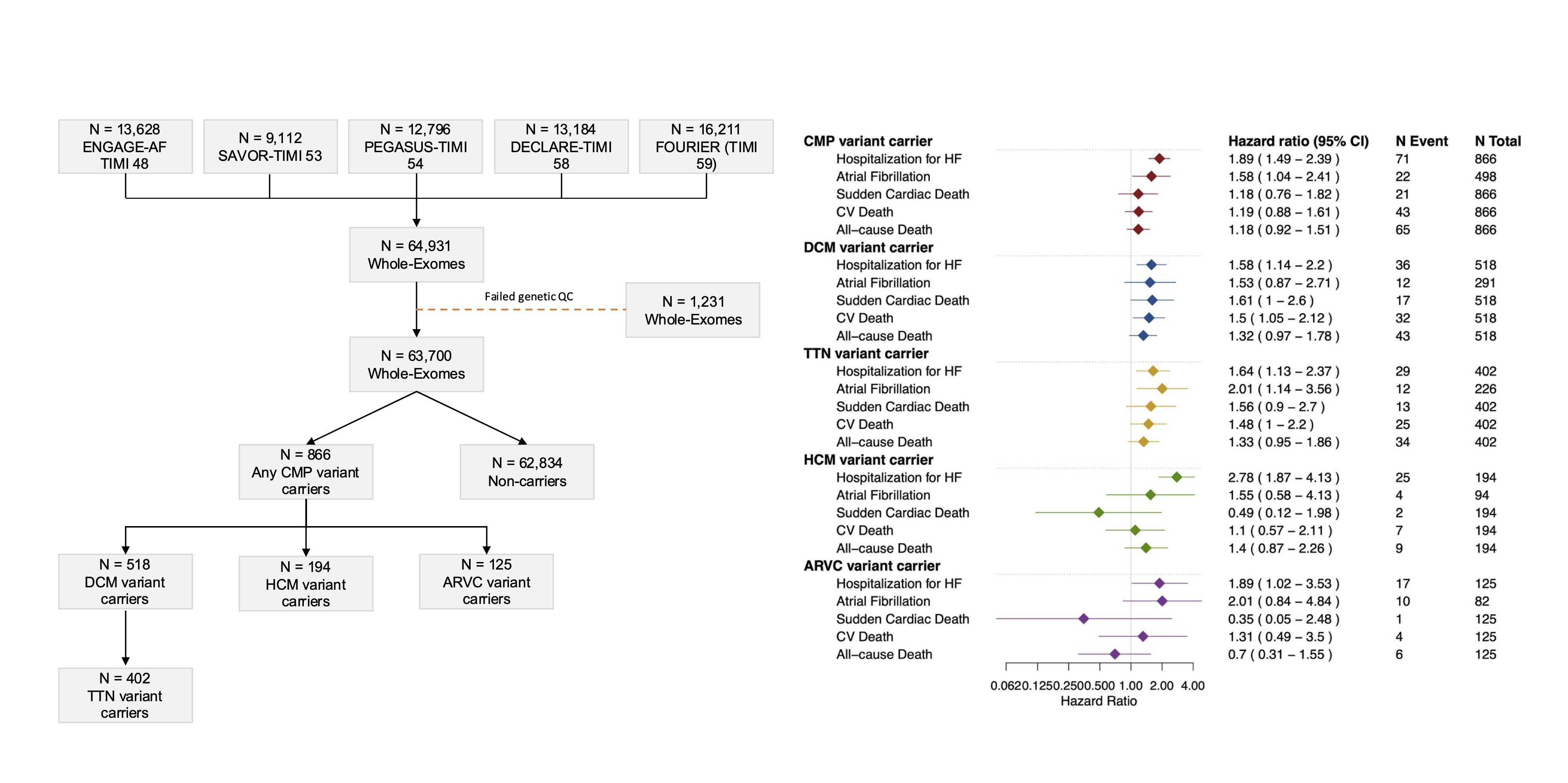
Exome sequencing data from five large multinational CV outcome trials (ENGAGE AF–TIMI 48, SAVOR–TIMI 53, PEGASUS–TIMI 54, DECLARE–TIMI 58, and FOURIER [TIMI 59]) were analyzed. Rare PLP variants were identified using phenotype- and gene-specific curation of protein-truncating variants and high-confidence ClinVar classifications. Logistic regression was used to assess associations with prevalent HF, and Cox proportional hazards models to assess incident HHF, adjusted for age, sex, trial, and the first ten principal components. Participants without CMP variants served as the reference group. Analyses were stratified by baseline HF status.
Results
Among 63,700 participants, 866 (1.4%) carried a CMP variant: 518 DCM (including 402 with a TTN variant), 194 HCM, and 125 ARVC. Mean age was 65±9 years; 69% were male. DCM variant carriers had higher odds of prevalent HF (odds ratio [OR] 1.94, 95% CI 1.57–2.39, p<0.0001), while associations for HCM (OR 1.18, 0.85–1.65) and ARVC (OR 1.23, 0.80–1.90) were not significant. Over a mean 2.5-year follow-up, HHF rates were higher among DCM (hazard ratio [HR] 1.58, 1.14–2.20, p=0.006), HCM (HR 2.78, 1.87–4.13, p<0.001), and ARVC (HR 1.89, 1.02–3.53, p=0.04) variant carriers. Associations were stronger among those without baseline HF (HR 2.06, 1.30–3.25) compared with those with HF (HR 1.48, 1.12–1.95). DCM variant carriers also had higher CV mortality (HR 1.50, 1.05–2.12, p=0.02), a pattern not observed in HCM or ARVC.
Conclusions
In five contemporary CV outcome trials, CMP variant carriers had higher rates of HF hospitalization, with DCM variant carriers also showing increased CV mortality. These results highlight the clinical importance of genetic stratification in CV trials and support the integration of genomic data to improve risk assessment and outcome prediction in cardiovascular disease.
Figure 1: Study overview and incident outcomes by carrier group