Background:
Different pulsed field ablation (PFA) systems for atrial fibrillation (AF) ablation have shown favorable acute efficacy and safety for pulmonary vein isolation (PVI). However, long-term comparative data between PFA catheters remain limited, particularly for additional ablation beyond PVI such as left atrial roof line ablation (LARA) and cavotricuspid isthmus (CTI) ablation.
Objective:
To compare 1-year clinical efficacy, safety, and procedural characteristics of pentaspline versus circular PFA catheters for fluoroscopy-guided PVI, LARA, and CTI ablation.
Methods:
Consecutive patients undergoing PVI with either pentaspline or circular PFA catheters between November 2023 and November 2024 were included. LARA was performed in patients with persistent AF and enlarged left atrium (LA area >20 cm²), and CTI ablation in those with typical atrial flutter (AFL). The primary endpoint was freedom from atrial arrhythmia (AF/AFL/AT) after a 3-month blanking period. Follow-up included scheduled visits, ECGs, Holter monitoring, and symptom-driven event recordings.
Results:
A total of 200 patients (65% male, 44% persistent AF, median age 66 [IQR 59–74] years) were included, 100 per group, with no baseline differences. LARA was performed in 30% of pentaspline (median 8 applications) and 32% of circular PFA cases (median 10 applications; p = 0.84), and CTI ablation in 3% (median 15 applications) vs. 5% (median 6 applications; p = 0.72). Acute bidirectional block was confirmed in all lines, and PVI success was 100% in both groups. Procedural and fluoroscopy times were comparable (63.0 [IQR 54–76.5] vs. 67 [IQR 58.8–80.3] min, p = 0.06; 11.9 [IQR 9.8–15.2] vs. 13.2 [IQR 10.2–15.9] min, p = 0.20).
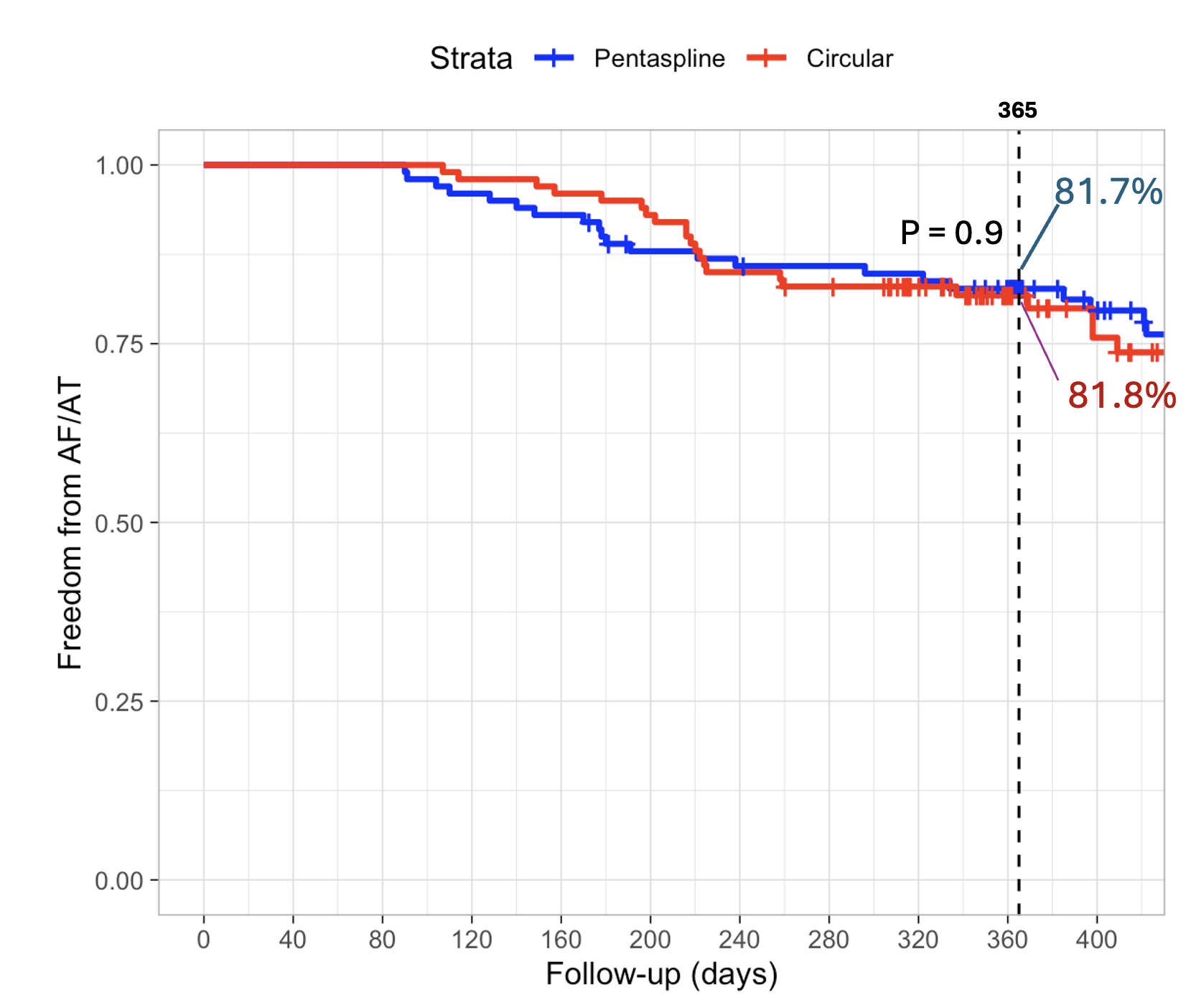
Median follow-up was 386 [IQR 349–486] days. At 1 year, Kaplan–Meier estimated arrhythmia-free survival was 81.7% vs. 81.8% (pentaspline vs. circular PFA; log-rank p = 0.90; Fig. 1), with similar success in paroxysmal AF (82.2% vs. 84.3%; p = 0.70) and persistent AF (80.6% vs. 78.7%; p = 0.90). In the PVI + LARA subgroup, 8/30 and 13/32 patients reached the endpoint (p = 0.37).
Redo procedures were performed in 20 patients (13 vs. 7, p = 0.24); residual roof line block was found in 2/4 vs. 1/2 cases, respectively. Two redo procedures involved CTI reablation for recurrent AFL, one in each group.
After univariate and multivariate analyses, early recurrence during the 3-month blanking period (HR 3.18, p < 0.001) and time since first AF diagnosis (HR 1.005, p = 0.004) independently predicted long-term recurrence. Overall complications were similar (5% vs. 3%, p = 0.72).
Conclusion:
Both pentaspline and circular PFA catheters demonstrated comparable procedural performance, safety, and 1-year arrhythmia-free survival for PVI and additional lesions (LARA and CTI), supporting the feasibility of comprehensive atrial ablation using PFA. Larger multicenter studies are warranted to confirm these findings and determine long-term lesion durability.