BackgroundSingle-shot pulsed-field ablation (PFA) systems have emerged as a promising alternative to cryoballoon (CB) ablation, enabling additional efficient lesion formation beyond pulmonary vein isolation (PVI), such as left atrial roof line ablation (LARA) in challenging cases of persistent atrial fibrillation (AF). However, comparative long-term data between CB and PFA single-shot technologies remain limited, particularly regarding the durability of roof line lesions and predictors of arrhythmia recurrence.
ObjectiveTo compare 1-year efficacy, safety, and predictors of arrhythmia recurrence after PVI combined with LARA using either cryoballoon ablation or pulsed field ablation (PFA) - performed with pentaspline or circular catheters - in patients with persistent atrial fibrillation and a dilated left atrium.
MethodsConsecutive patients with persistent AF and left atrial enlargement (LA >20 cm²) undergoing first-time PVI with LARA using CB, pentaspline, or circular PFA catheters were analyzed. Follow-up included scheduled clinic visits, ECGs, Holter monitoring, and symptom-triggered event recordings. Arrhythmia recurrence was defined as any atrial tachyarrhythmia >30 s after a 3-month blanking period. Both PFA catheter types were analyzed as one PFA group for energy-source comparison.
Results A total of 125 patients were included (CB 65; PFA 60 [pentaspline 30; circular 30]). Median age was 67 (IQR 61-74) years, BMI 29 (IQR 26-32) kg/m², and LA area 25 (23-29) cm². Procedural time was longer with CB than PFA (87 [IQR 76–99] vs. 67 [IQR 63–83] min, p < 0.001), while fluoroscopy time was shorter (12.2 [IQR 9.6–15.3] vs. 15.2 [IQR 12.4–16.7] min, p < 0.001). Roof line applications/freezes were 4 (IQR 4–5) in CB vs. 8.5 (IQR 7–12) in PFA (p < 0.001), with confirmed conduction block in 95% and 100%, respectively. Acute PVI success was 100% in both groups.
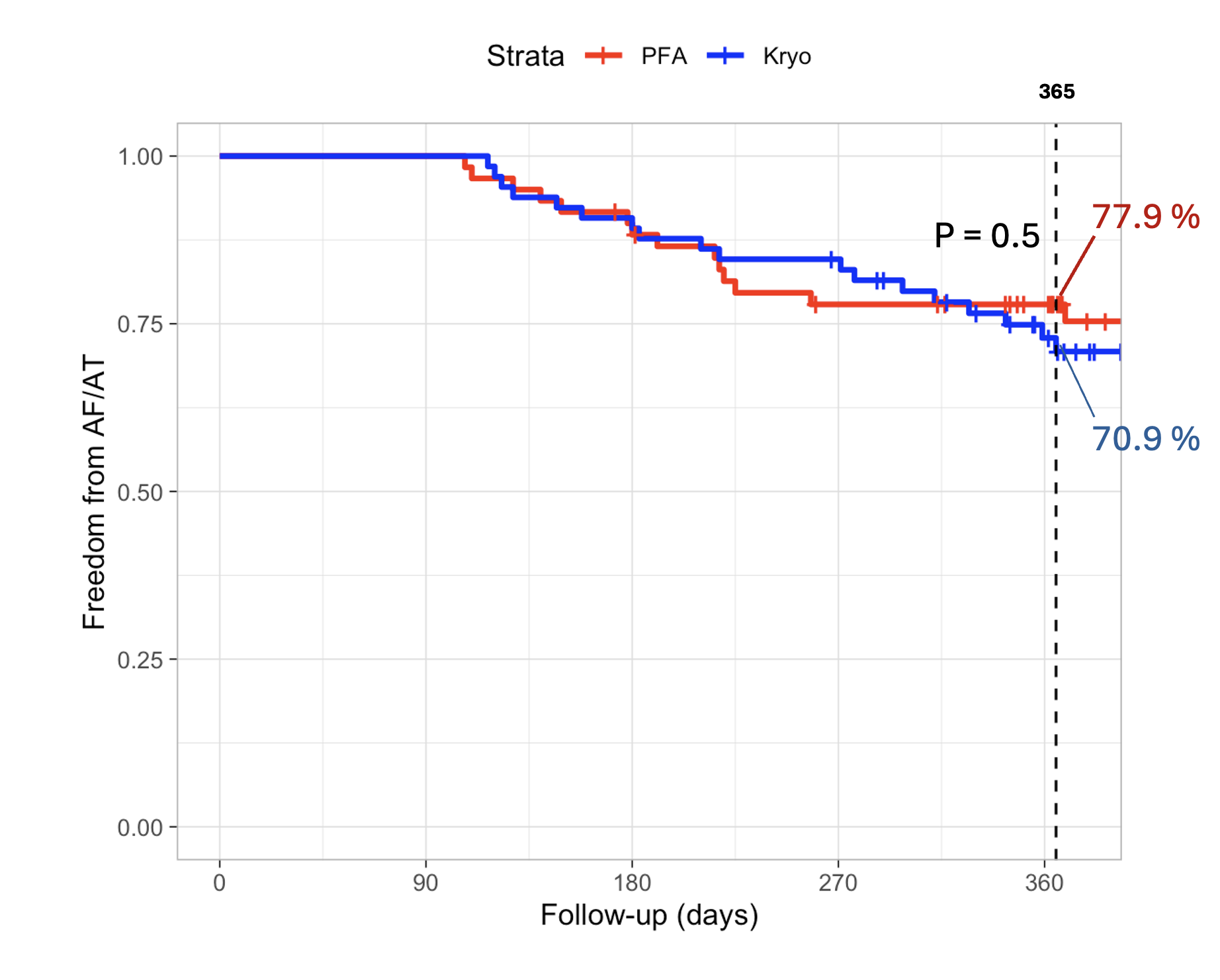
Median follow-up was 393 days (IQR 348–504). At 1 year, Kaplan–Meier–estimated arrhythmia-free survival was 70.9% in CB and 77.9% in PFA (log-rank p = 0.5; Figure 1), with no significant difference among the three ablation systems (CB, pentaspline PFA, circular PFA; p = 0.55). Reablation was performed in 4/65 (6.2%), 4/30 (13.3%), and 2/30 (6.7%) patients in the CB, pentaspline, and circular PFA groups, respectively, with roof line still blocked in 3/4, 2/4, and 1/2 cases.
Only early recurrence during the 3-month blanking period predicted long-term AF recurrence (HR 5.17, 95% CI 2.69–9.94, p < 0.001); all other variables, including energy source and LA area, were not significant. Overall complications were similar between CB and PFA (4 vs. 1; p = 0.37), including one transient phrenic nerve palsy in the CB group and other vascular events.
ConclusionAt 1-year follow-up, CB and PFA catheters demonstrated comparable efficacy and safety for combined PVI and roof line ablation in patients with persistent AF and left atrial dilatation, with PFA showing shorter procedural but slightly longer fluoroscopy times. Multicenter studies are warranted to confirm these findings.