Background The baroreflex plays a crucial role in blood pressure (BP) regulation, and its dysfunction is one cause of hypertension. Baroreflex activation therapy (BAT) works via electric stimulation of the baroreceptors in the carotid sinus and has been shown to reduce BP, but long-term data are limited.
Methods Patients treated with BAT for resistant hypertension for ≥3 years, in a routine outpatient setting, were included in this retrospective single-center study. Office BP and antihypertensive medication were documented at each visit, ambulatory BP was used when available.
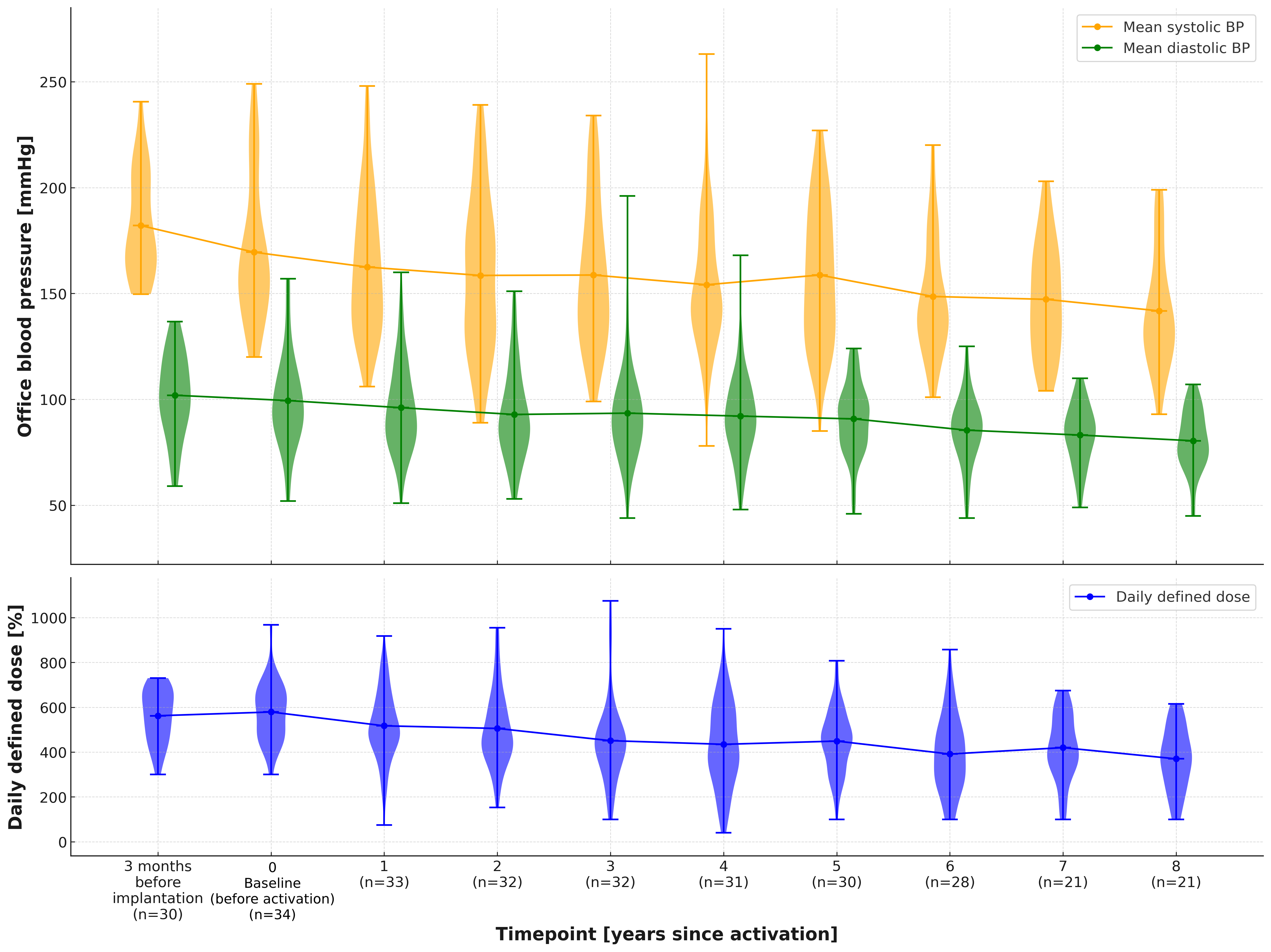
Daily defined doses (DDD) were calculated, with 100% being the recommended maximum dose of one substance. Echocardiographic parameters were compared when available. Statistical analysis using paired, one-tailed t-tests for assessing mean differences between baseline and follow-up, was considered significant at p<0,05. Independent two-tailed t-tests were used for comparing BP reductions in patients without and with prior renal denervation (RDN). Data are normally distributed and are presented as mean ± standard deviation.
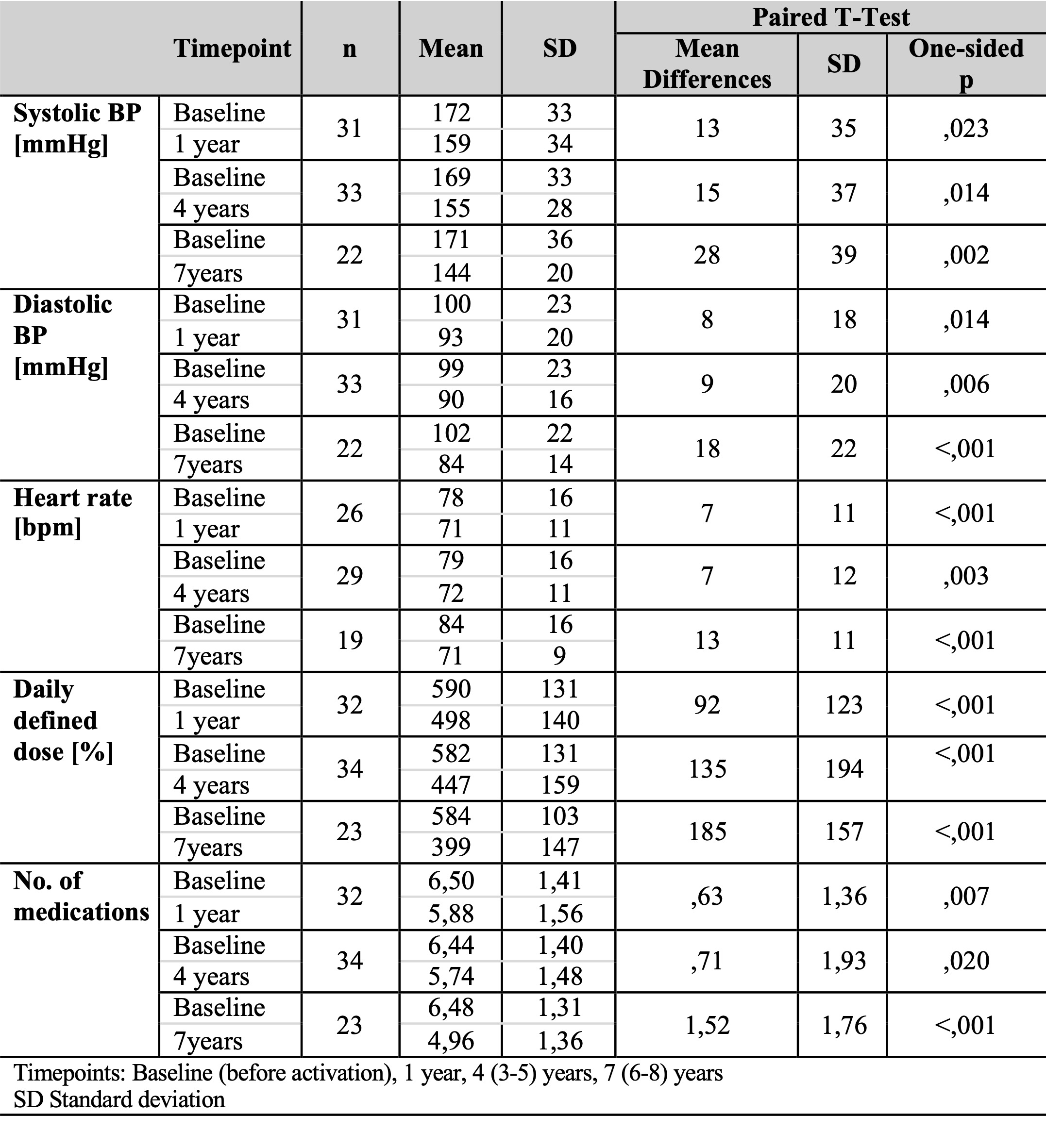
Results 34 patients were included, mean follow-up was 8,1 years (3,3 to 14,8 years). We compared baseline (last visit before activation, i.e. after implantation of the device) with mean values after 1 year, 4 (3-5) years, and 7 (6-8) years and found a significant reduction of office systolic BP (SBP), diastolic BP (DBP), and heartrate (HR) (Tbl.1). We also observed a BP reduction between implantation and activation (Fig.1). DDD and number of medications were significantly reduced comparing baseline vs 1, 4 and 7 years (Tbl.1).
Comparing patients without and with prior RDN, there was no significant difference in the mean reduction of office BP between baseline and the last visit (no RDN n=18 vs RDN n=15; SBP –21±41 mmHg vs -18±48 mmHg, p=0,820; DBP -15±24 mmHg vs -13±22 mmHg, p=0,844).
After 4 years, 91% had either a ≥5mmHg reduction of office BP or ≥15% of their DDD and 53% had a reduction of both BP ≥5mmHg and DDD (n=34). After 7 years, 30,4% of patients achieved optimal BP control ≤130 mmHg compared to 5,9% at baseline. Interventricular septal diameter, left ventricular ejection fraction and E/E’ remained stable (IVSd n=23, LVEF n=20, E/E’ n=15, mean follow-up 5,38 years).
Conclusion Chronic BAT significantly reduces office and ambulatory BP and decreases the necessary number and DDD of antihypertensive medication, showing the potential to reduce polypharmacy. With a high responder rate, BAT seems to be beneficial for most patients. Stable hypertension-related echocardiographic parameters suggest a long-term hemodynamic stability achieved through chronic BAT. With no significant difference in office BP reductions at the last visit comparing patients with and without prior RDN, BAT seems to have a positive effect even after RDN.