Background
Current heart‑failure guidelines rely on natriuretic peptides, especially NT-proBNP, to guide diagnosis and further testing. These peptides reflect myocardial stress, but a single “normal” threshold ignores the rich variability shaped by age, sex, body mass, kidney function, and rhythm. Currently, we lack robust data on how to weight these factors for an individual.
Aims
In the STAAB cohort, rigorously phenotyped population sample of Würzburg residents without heart failure, we aimed to identify independent determinants of NT-proBNP, construct age- and sex-specific reference percentiles, and derive a straightforward correction formula incorporating further determinants. The goal was a practical tool clinicians can use at the bedside.
Methods
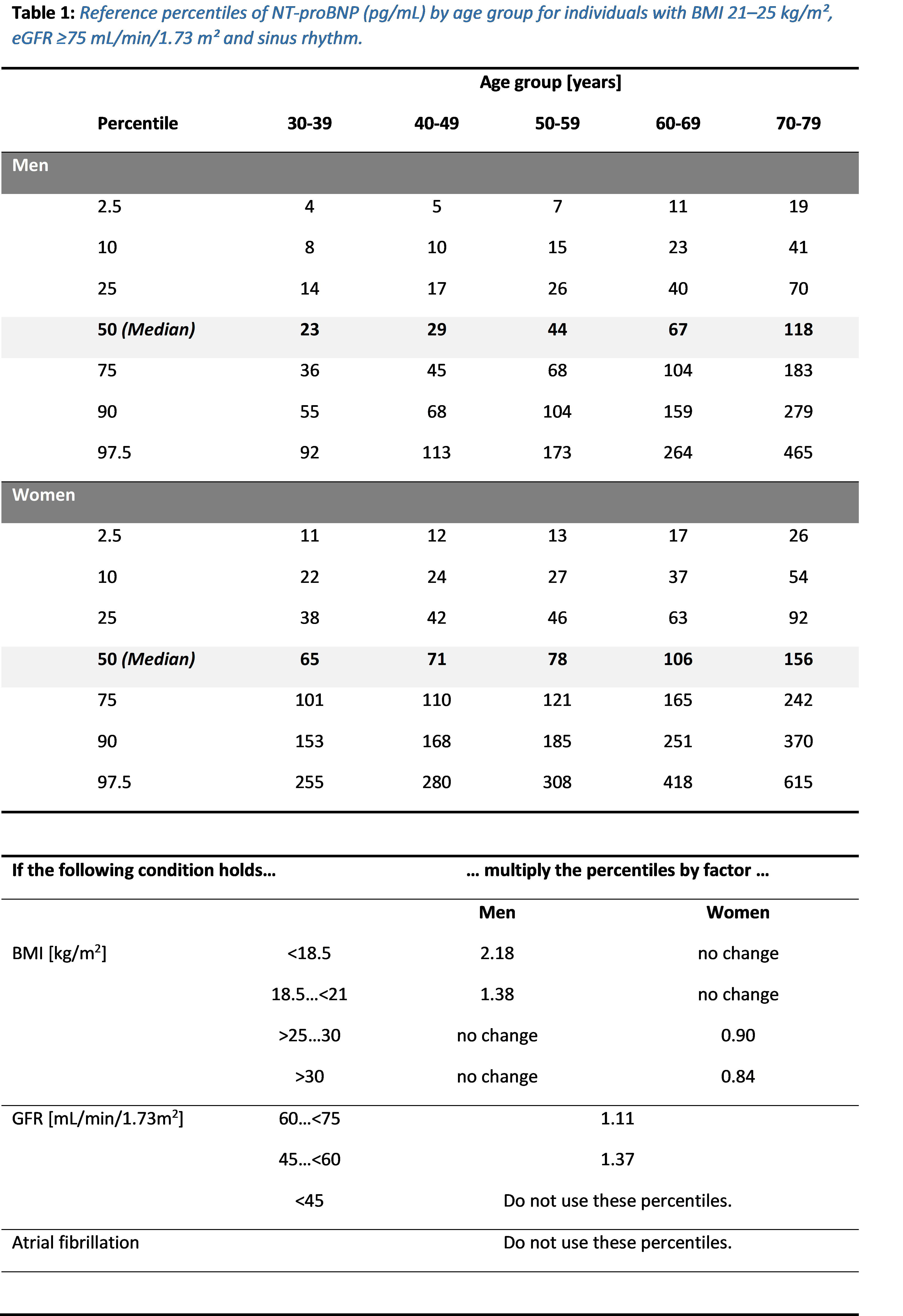
STAAB sampled 5.000 residents aged 30–79 years between December 2013 and October 2017 (2011 census population 124,297) stratified by sex and decade. Those without prior heart failure diagnosis underwent detailed surveys, examinations and blood draws; NT-proBNP was assayed centrally. We modelled log-transformed NT-proBNP against age, sex, BMI (WHO categories), eGFR bands, and heart rhythm (sinus vs non-sinus) using multivariable linear models, and testing sex-by-age and sex-by-BMI interactions. We defined a “reference” subgroup (BMI 21–25 kg/m², eGFR ≥75 mL/min/1.73 m², sinus rhythm) to compute percentiles, then derived multiplicative factors to adjust for other BMI and eGFR strata and for atrial fibrillation. Individuals with multiple deviations multiply the relevant factors sequentially.
Results
NT-proBNP rose markedly with age in both sexes. Women had higher values at all ages, yet men’s steeper age-related increase narrowed the sex gap in older decades (i.e, the women-to-men ratio dropped from 2.8 at ages 30-39 to 1.26 at ages 70-70 years). Underweight men (BMI <18.5 kg/m²) had more than double the levels of normal-weight men, whereas in women this association disappeared. Conversely, overweight and obese women had NT-proBNP about 10% and 17% lower than normal-weight women; elevated BMI hardly changed values in men. Renal function had a dose-dependent effect with higher NT-proBNP in lower eGFR categories. Atrial fibrillation was linked to a 3.5-fold increase over sinus rhythm. Based on these determinants, we tabulated sex- and age-specific percentiles (Table) and provided correction factors.
Conclusion
NT-proBNP is not a one-size-fits-all marker; it varies systematically with age, sex, body habitus, and renal function. By offering percentiles anchored in a reference population and correction factors for key covariates, our work allows NT‑proBNP interpretation to be tailored to the individual. Such personalised thresholds could reduce unnecessary testing and avoid missed diagnoses in daily practice. Prospective validation is warranted.