Background and aim
Infiltrative cardiomyopathies are characterized by pathological deposition of proteins or metabolites within the myocardium, leading to left ventricular (LV) hypertrophy and progressive myocardial dysfunction. Myocardial Work (MyW) analysis, derived from non-invasive, echocardiography-based pressure–strain loops, offers a load‑adjusted measure of ventricular performance that may provide additional diagnostic granularity beyond LV ejection fraction and global longitudinal strain (GLS). We hypothesized that the principal infiltrative cardiomyopathies—transthyretin (ATTR) amyloidosis, light-chain (AL) amyloidosis, and Fabry disease—exhibit distinct MyW profiles.
Methods
This retrospective analysis included patients with infiltrative cardiomyopathies enrolled in the PAVE (pathology-focused automated quantification of echocardiography) study at the Comprehensive Heart Failure Center, and patients from the Fabry Center, both located at the University Hospital Würzburg. MyW analysis was performed from stored echocardiography images using EchoPac 202 (GE, Norway). Intergroup comparisons were performed using the Kruskal–Wallis test followed by Bonferroni-adjusted pairwise post-hoc comparisons.
Results
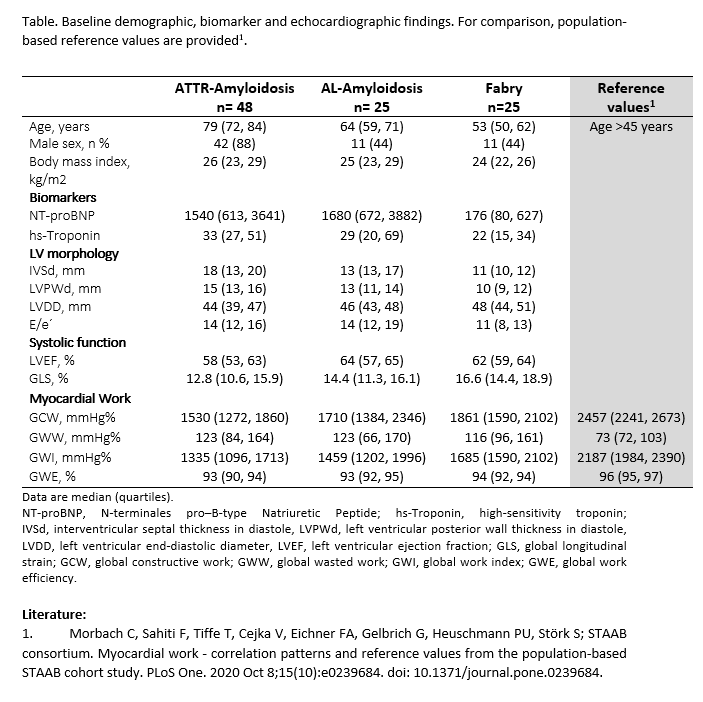
Among 108 patients analyzed, 48 had ATTR amyloidosis, 25 had AL amyloidosis, and 25 had Fabry disease. Baseline demographic, laboratory, and echocardiographic characteristics of the study population are summarized in the Table. Among the three infiltrative cardiomyopathy subgroups, significant intergroup effects were observed for GLS (p<0.001), global constructive work (GCW; p=0.003), and global work index (GWI; p<0.001). Global work efficiency (GWE) showed a borderline difference (p=0.073), while global wasted work (GWW) did not differ among groups (p=0.780). Post-hoc pairwise comparisons with Bonferroni adjustment demonstrated that patients with ATTR amyloidosis had significantly lower GLS, GCW, and GWI compared to those with Fabry disease (p≤0.002 for all). Although median values for AL amyloidosis mirrored those seen in the ATTR cohort, differences versus Fabry disease did not remain significant after correction. No significant differences were observed between AL and ATTR amyloidosis.
Conclusions
Non‑invasive MyW analysis uncovers subtle yet clinically relevant differences in myocardial performance among infiltrative cardiomyopathies with preserved ejection fraction. In relation to contemporary reference values1, all patient groups exhibited uniformly elevated wasted work and markedly reduced constructive work. The reduction of GCW and GWI was more pronounced in patients with amyloidosis when compared to patients with Fabry disease. Our results encourage the incorporation of MyW metrics in the diagnostic evaluation of myocardial storage diseases but require confirmation in larger cohorts.