Case History:A 39-year-old woman presented with progressive exertional dyspnoea and palpitations over several months. Her medical history included childhood asthma and active nicotine use.
Examination Findings:On physical examination, a grade 3/6 systolic murmur was heard at Erb’s point; there was no peripheral edema, and blood pressure was 140/60 mmHg. Laboratory testing revealed a mildly elevated BNP, with no anemia or thyroid dysfunction. Resting ECG showed sinus rhythm at 93 bpm with P mitrale and a positive Sokolow–Lyon index. Echocardiography demonstrated enlargement of all four cardiac chambers (LV 68/42 mm; Fig. 1a, 1e), increased transvalvular flow velocities (aortic 2.6 m/s), an estimated systolic pulmonary artery pressure of 55 mmHg, and a markedly dilated inferior vena cava (4.5 cm).
Cardiac magnetic resonance imaging (MRI) confirmed a 30% increase in total heart volume (1150 mL) with no late gadolinium enhancement (Fig. 1b). Flow measurements over aorta and pulmonary artery were equal.
Cardiac catheterization showed a normal coronary angiogram. The expected hemodynamics for a 39-year-old woman (171 cm, 88 kg, heart rate 77/min) would be a cardiac output of 5,4 l/min with a stroke volume of 70 ml. Our patient had a stroke volume of 152 ml and
cardiac output was 11.5 L/min. Peripheral vascular resistance was low at 905 dyn·s/cm⁵ (normal 900–1400), and pulmonary vascular resistance was high normal at 89 dyn·s/cm⁵ (normal 45–120). The systolic pulmonary artery pressure was 50/17 mmHg. The oxygen saturation was 66% in the superior vena cava and 95% in the inferior vena cava. Invasive blood pressure measurement (120/34 mmHg) revealed a low diastolic value.
Given the high oxygen saturation in the inferior vena cava and the low diastolic pressure, abdominal MRI was performed, revealing a high-flow fistula between the right iliac artery and vein (Fig. 1c).
Therapy:Via the left femoral artery, the right internal iliac artery was initially occluded using two 8 mm Amplatzer Vascular Plugs IV (crossover technique) to prevent a type II endoleak. Subsequently, through the right femoral artery, the arteriovenous fistula was closed with two overlapping covered stents. Follow-up CT after four weeks confirmed complete occlusion of the fistula (Fig. 1d).
Discussion:Iliac arteriovenous fistulas are rare. They typically with aortic aneurysms or after lumbar disc surgery. Diagnosis is often delayed, and the resulting shunt may cause high-output heart failure. Endovascular closure with covered stents represents the treatment of choice and can be performed safely even in emergency situations. In this patient, interventional closure resulted in rapid clinical improvement with normalization of diastolic blood pressure and reduced heart rate. On echocardiographic follow up after four years a normalisation of cardiac output (aortic flow velocity 1,2 m/s) and regression of chamber dilatation (LV 49/32 mm, Fig 1f) could be documented. This case demonstrates the complete recovery from heart failure after treatment of the underlying shunt fistula.
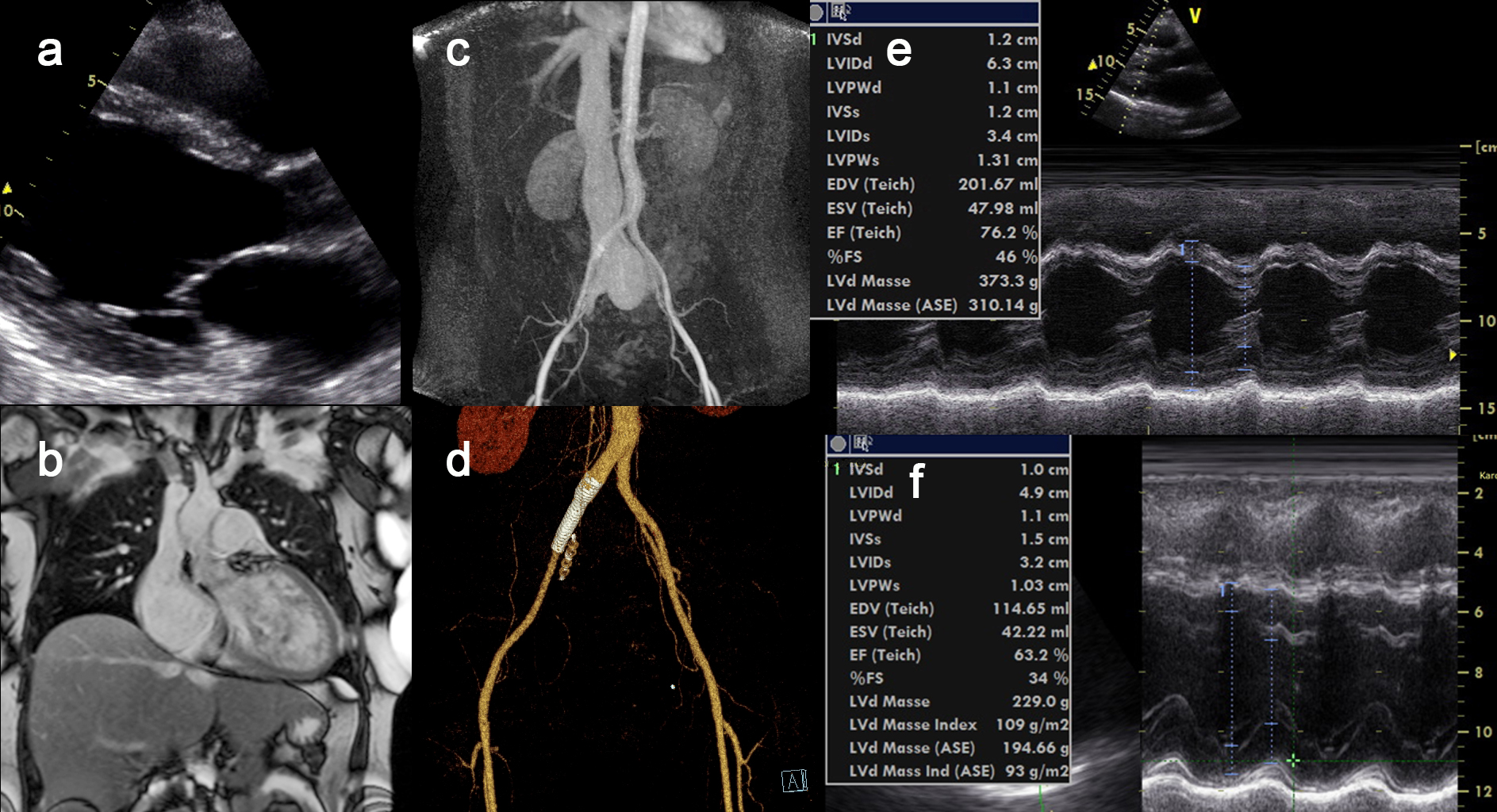
Figure 1: Complete normalisation of cardiac function in high volume heart failure after closure Iliac arteriovenous fistula



