Case Presentation: A 76-year-old smoker presented with typical angina. Echocardiography revealed anteroseptal and anterior hypokinesia. Relevant comorbidities included carotid sclerosis, permanent atrial fibrillation, and a history of right hemicolectomy for colon carcinoma.
Angiography:
Coronary angiography demonstrated diffuse three-vessel disease. A calcified nodule was identified in the left main coronary artery (LMCA), extending into the proximal left anterior descending artery (LAD). The LAD exhibited a heavily calcified subtotal mid-segment stenosis involving the diagonal branch (Fig. 1a). The marginal branch showed 75% stenosis, while the right coronary artery (RCA) demonstrated 75% mid and 90% distal tandem stenoses. Following discussion in the heart team conference, an interventional approach was chosen.
Therapy:
Cardiac catheterization was performed via the right radial artery (Fig. 1a). After placement the guidewire in the distal LAD, intravascular ultrasound (IVUS) was performed and confirmed the presence of a calcified nodule extending from the left main coronary artery (LMCA) into the proximal LAD (Fig. 1b).
Initial lesion preparation was achieved by multiple passes of a 1.5 mm rotablation burr through the LMCA and proximal to mid LAD (Fig. 1c). The preparartion with rotablation ensured continuous flow through the left main and LAD, avoiding the need for circulatory support.
Due to the persistence of significant plaque burden in the LMCA, intravascular lithotripsy was subsequently performed using a 2.5 mm Shockwave balloon, followed by dilation with a 3.5 mm balloon (Fig. 1d). A second guidewire was then advanced into the marginal branch, and the LMCA bifurcation was treated using the double-kissing crush technique (Fig. 1e). Final proximal optimization technique was applied using a 4.5 mm non-compliant balloon at 22 bar under IVUS guidance, achieving an excellent angiographic result (Fig. 1f).
The procedure duration was 130 minutes, with 200 mL of contrast used and a radiation dose of 3230 cGy·cm².
On the following day, the severely calcified RCA was treated with rotablation, high-pressure ballooning, and implantation of four drug-eluting stents. The patient was discharged the next day, symptom-free, with a peak creatine kinase level of 218 U/L.
Discussion: Calcified coronary stenoses are becoming increasingly common in older patients. In this case, we performed an intervention on an unprotected left main artery without a circulatory support system. Lesion preparation through rotablation and subsequent lithotripsy consistently maintained flow within the left main coronary artery. Through use of a high interventional effort, including the use of high-pressure balloons and multiple stent implantations in the right coronary artery, we were ultimately able to achieve an almost complete revascularization within a short hospital stay.
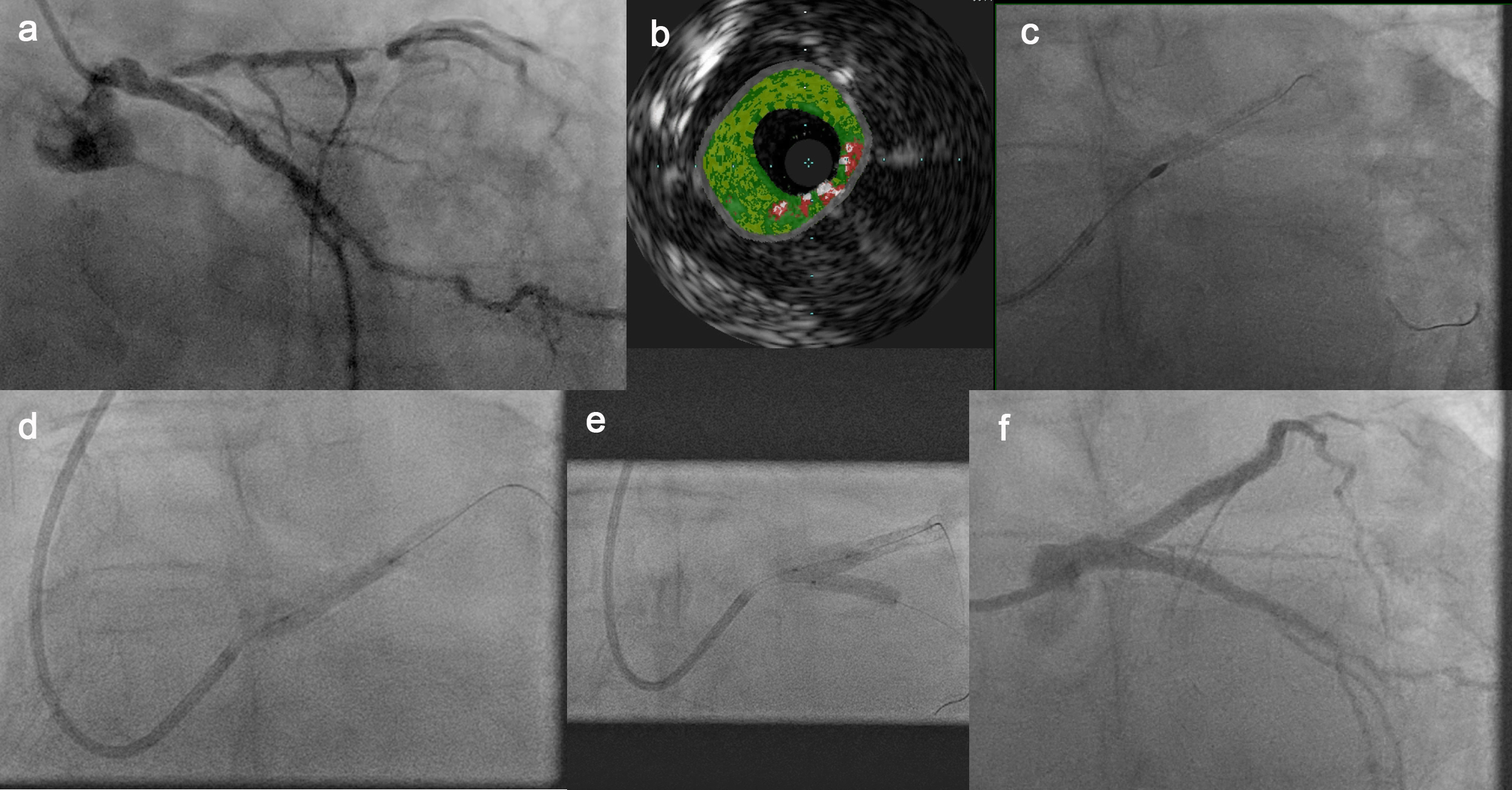
Figure 1: Interventional treatment of a calcified nodule in an unprotected left main coronary artery using a combination of intravascular ultrasound, rotablation and lithotripsy



