Introduction: Congenital absence of the pericardium is a rare disorder. While the majority of cases are asymptomatic, the most feared complication is myocardial ischemia due to cardiac strangulation across a partial defect of the pericardium. In this case, the patients present with both Myocardial Infarction with Non-obstructive Coronary Arteries (MINOCA) and pericardial aplasia, a complex clinical picture where an acute heart attack occurs without significant preexisting coronary artery disease, and the protective outer sac of the heart is partially absent.
Presentation Case: A 53-year old woman presented with chest pain to the emergency room. Troponin was positive. The ECG showed complete left bundle brunch block. The chest x ray demonstrated levocardia of the heart. Cardiac catherization showed smooth unobstructed coronaries with normal anatomy. However, ejection fraction (EF) was extremely reduced with an EF of 20%. Myocardial biopsy showed no evidence of myocarditis or dilated cardiomyopathy.
One month later the patient underwent cardiac MR imaging which showed the typical signs of pericardial agenesis: extreme levocardia of the heart resulting in elongation and ectasia of the aorta and pulmonary artery, interposition of lung tissue between the diaphragm and the base of the heart and increased cardiac mobility (‘swinging heart’). The late enhancement (LGE) revealed transmural scarring and hypo- and akinesia of the anterior wall.
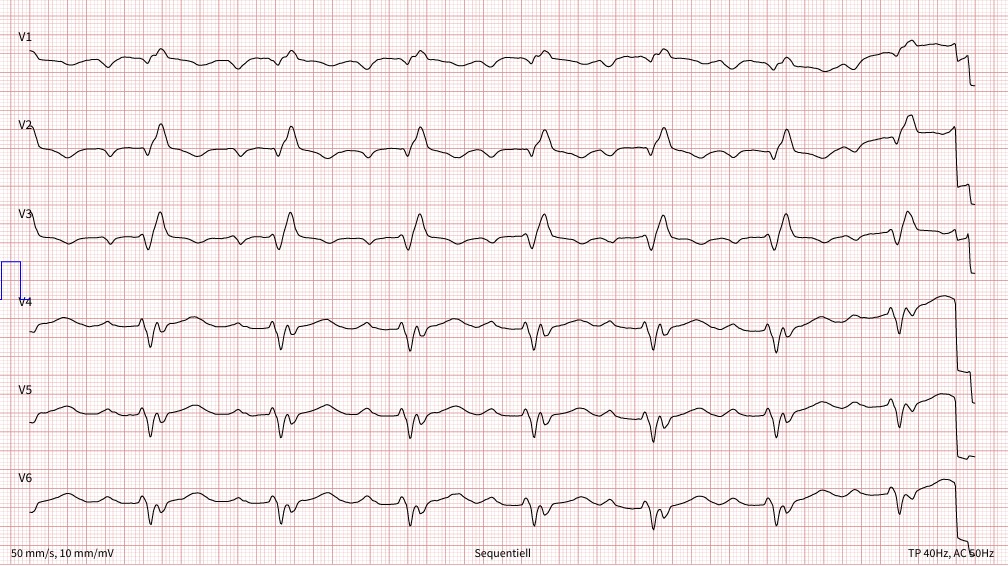
The patient received pharmacological treatment for heart failure with reduced ejection fraction. The recommendation to implant a defibrillator due to persistence of severely impaired systolic LV-function of 35% was rejected by the patient. Follow-Up ECG after two years showed a Q wave and R loss over the entire anterior wall (V1-V6) as a sign of a previous anterior wall infarction.
Conclusion: Pericardial agenesis should be suspected in patients with marked levoposition of the cardiac silhouette, loss of right heart border, prominent pulmonary artery and lung tissue interposing between main pulmonary artery and aorta as well as between the heart and spine. The main complications are herniation and compression of the left coronary artery.
Fig 1: MRI: levoposition of the cardiac silhouette, prominent pulmonary artery, and lung tissue between the diaphragm and inferior border of the heart
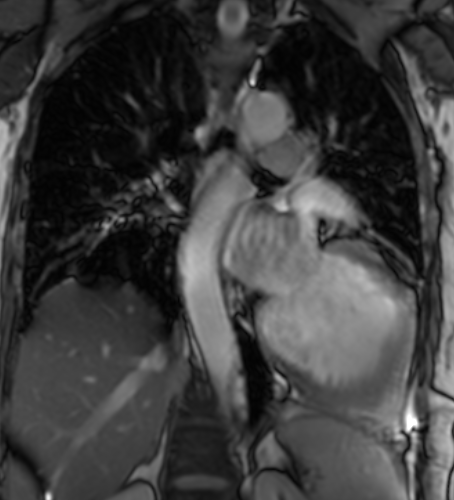
Fig 2: MRI: transmural LGE of the anterior wall
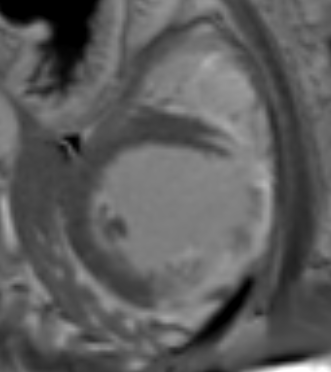
Fig 3: CT: displacement of the heart with the trachea remaining in the middle, and interposition of the lung between the diaphragm and inferior border of the heart

Fig 4: Cardiac catherization: smooth unobstructed coronaries

Fig 5: CT: RIVA in close spatial relation to the chest wall
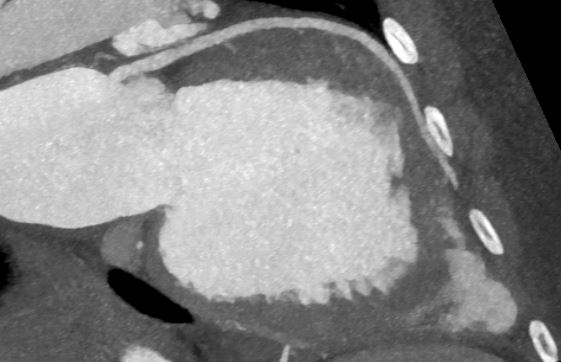
Fig 6: ECG: anterior wall infarction