Background: Elevated cardiac filling pressures are a key feature of adverse outcome after acute myocardial infarction (AMI). Recently, a cardiovascular magnetic resonance (CMR)-modelled postcapillary wedge pressure (PCWP) estimation has been introduced, but data on its diagnostic and prognostic implications are scare. We hypothesized, that CMR PCWP would enable risk stratification beyond conventional CMR parameters and cardiovascular risk factors.
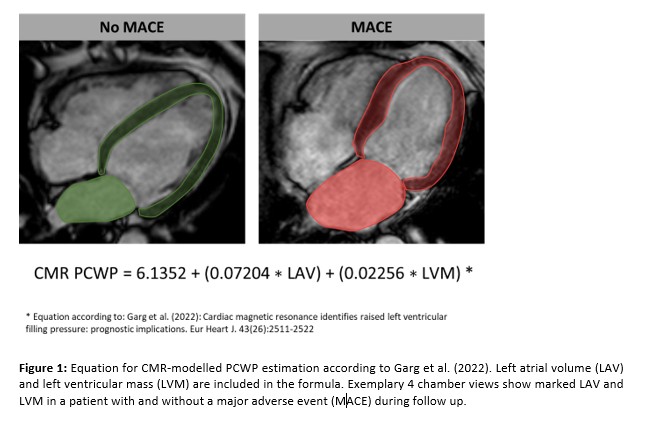
Methods: A total of 1046 AMI patients were included in this study. CMR imaging was performed after primary percutaneous coronary intervention. Comprehensive image analyses included assessment of myocardial function and infarct characteristics. CMR-modelled PCWP was calculated based on a previously published equation including left ventricular (LV) mass and left atrial volume (Figure1). Primary clinical endpoint of the study was the occurrence of major adverse cardiac events (MACE) including death, reinfarction or congestive heart failure within 12 months after infarction.
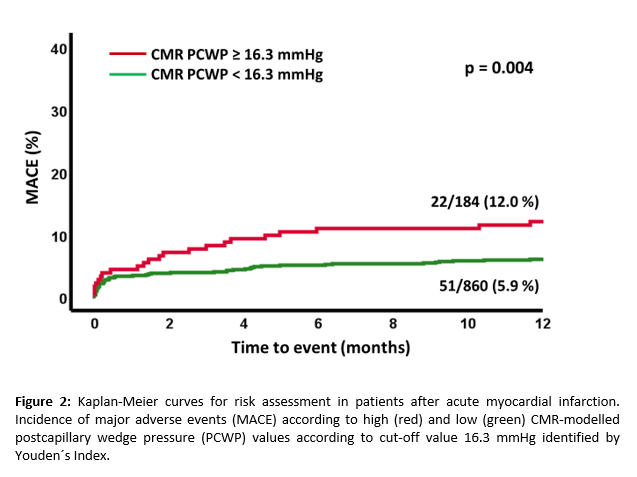
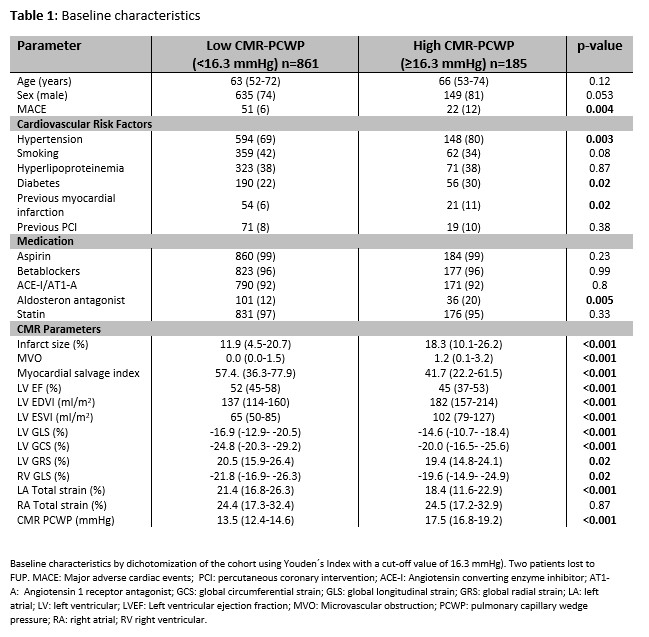
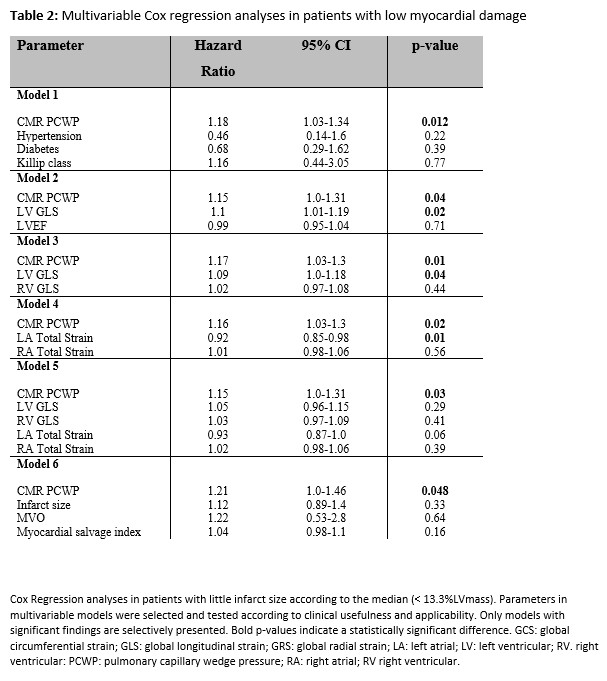
Results: Youden Index identified an optimal PCWP cut-off at 16.3mmHg to classify patients at high-risk (p=0.004 on log-rank testing)(Figure2). Dichotomizing the cohort into patients with high and low PCWP (≥/ <16.3mmHg), there were no differences in age (p=0.12) or sex (p=0.053) but higher presence of risk factors (diabetes: p=0.02, hypertension: p=0.003), impaired myocardial function (LV ejection fraction and strain) and larger infarct size (IS)(p<0.001 for all) in patients with higher PCWP (Table1). Higher PCWP was associated with MACE on univariate regression modeling (HR 1.12 95% CI 1.03 – 1.23, p=0.008). In patients with smaller IS according to the median (13.3%LVmass), CMR PCWP remained significantly associated with MACE on multivariate modeling independently from all strain values (HR 1.15 95% CI 1.0-1.31, p=0.03) or risk factors (Table 2).
Conclusion: CMR-modelled PCWP is associated with adverse outcome in patients following AMI. Especially in patients with smaller myocardial damage, CMR PCWP detects patients at higher risk for the occurrence of MACE and enables independent risk prediction.