BackgroundAvailable lipid-lowering therapies (LLT) effectively reduce LDL-C and cardiovascular risk; nevertheless, the majority of ASCVD patients fail to achieve the recommended LDL-C treatment targets. The disease management programme for coronary artery disease (DMP-CAD) was introduced in Germany in 2002. Contemporary data on potential benefits of this resource-intensive structured treatment programme regarding LLT utilisation are lacking.
MethodsThis analysis was based on the German Analysis Database for Evaluation and Health Services Research (DADB), encompassing health claims data for approximately 4.4 million individuals provided by 16 statutory health insurances. Additional area-based information on socioeconomic status was utilised from the INKAR database. Patients with diagnosed ASCVD (CAD, cerebrovascular disease, or peripheral artery disease) were included. The primary outcome was at least one prescription of LLT in 2023. Covariates for multivariable logistic regression analysis included cardiovascular risk factors and socioeconomic factors.
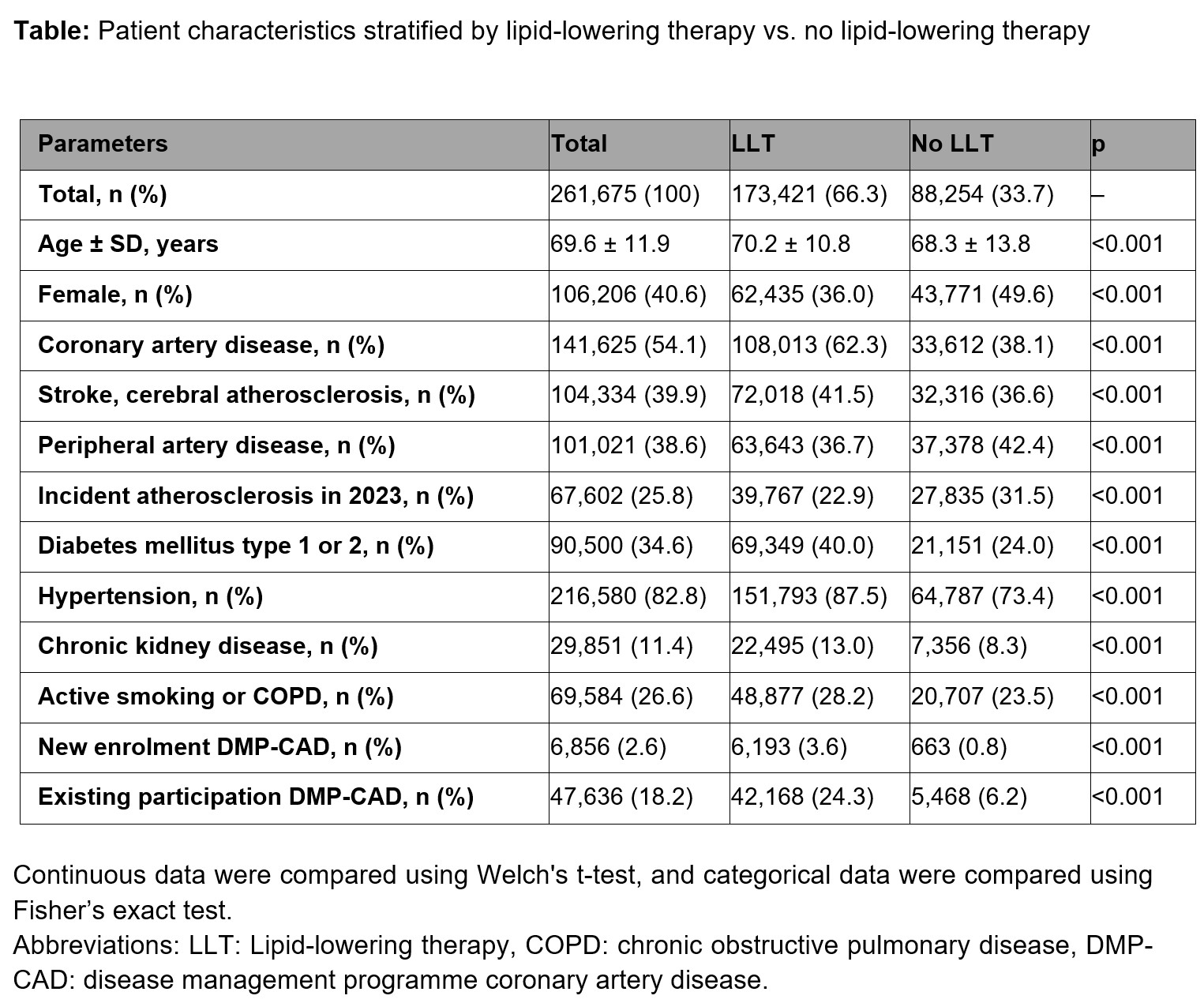
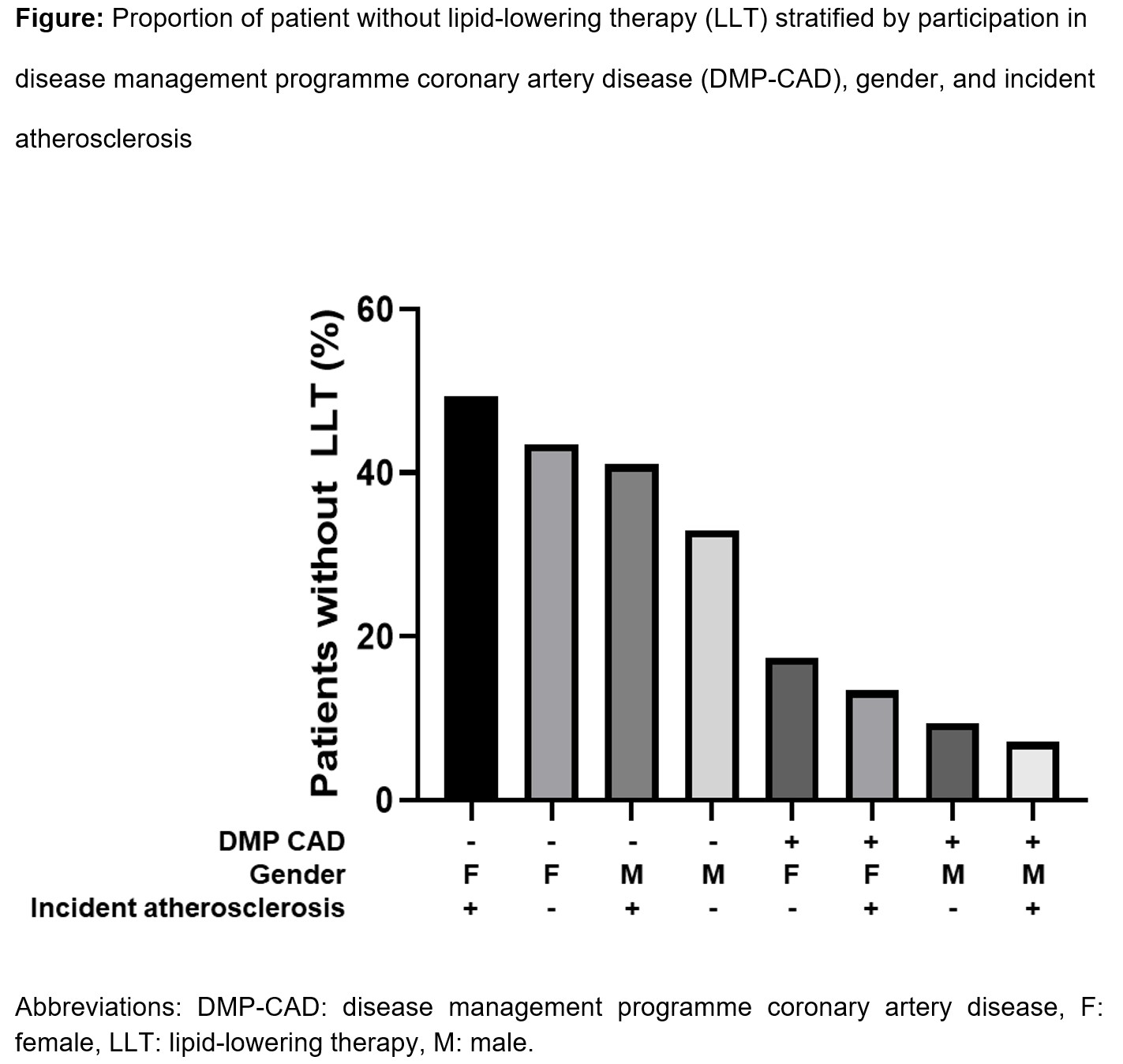
ResultsAmong the 2.8 million individuals in the database in 2023 with 2022 as baseline, 261,675 met the inclusion criteria. One in three patients (33.7%) did not receive any LLT, and 53.1%, 12.6%, and 0.5% received oral monotherapy (statin, ezetimibe, or bempedoic acid), oral combination LLT, and a PCSK9 inhibitor, respectively. Patients with LLT were slightly older, more often male, had more cardiovascular risk factors, and more frequently participated in the DMP-CAD (Table). Incident atherosclerosis in DMP-CAD participants was associated with more frequent LLT, whereas the opposite was observed in non-participants (Figure). In the multivariable analysis, the explanatory variables with the largest effect sizes for LLT prescription were existing or new participation in the DMP-CAD (adjusted odds ratios (aOR) [95% CI] 4.06 [3.94-4.19] and 5.74 [5.29-6.23], respectively). The next largest effect size was found for hypertension with an aOR (95% CI) of 1.90 (1.86-1.94), followed by other cardiovascular risk factors, and with small effect sizes, socioeconomic factors. The factors with the largest effect size for not receiving LLT were female gender (aOR [95% CI] 0.66 [0.65-0.67]) and incident atherosclerosis (0.81 [0.80-0.83]).
ConclusionsIn this large, contemporary cohort of 261,675 patients with diagnosed ASCVD, one-third of patients did not receive any lipid-lowering therapy. Among a comprehensive set of potential explanatory variables including factors reflecting socioeconomic status, participation in the DMP-CAD was the strongest predictor for receiving LLT. The present results strongly support the notion that participation in the DMP-CAD improves lipid management and call for early and consequent patient enrolment. Furthermore, our findings support a potential expansion of the scope of the DMP-CAD to atherosclerosis in vascular territories other than coronary.