Background and aimsAdherence and persistence to lipid-lowering therapies (LLT) have frequently been reported to be low over time. Gaps and re-initiation of treatment with LLT are however frequent. The cumulative exposure hypothesis states that the duration and magnitude of LDL cholesterol (LDL-C) elevation determine its impact on cardiovascular risk. Therefore, time on lipid-lowering agents may reflect the expected benefits from LLT. We aimed to investigate the longitudinal course of treatment with LLT, quantify treatment gaps, and estimate LLT coverage over time.
MethodsThis analysis was based on the “Deutsche Analysedatenbank für Evaluation und Versorgungsforschung” (DADB), administered by “Gesundheitsforen Leipzig GmbH”. The database contains health claims data from 16 statutory health insurers and covers about 4.4 million persons. Patients were included in this analysis if they received at least two LLT prescriptions (Table) between 2016 und 2023. Treatment gaps of >3 months after run-out of a claim were quantified, and LLT coverage, defined as the proportion of patients on active LLT on each reference day throughout the observation period, was calculated by an area-under-the-curve approach.
ResultsA total of 266,241 patients met the inclusion criteria. The mean age was 63.6 (SD, 11.9) years, 43.1% were female, 54.5% had ASCVD. The vast majority of patients received statin monotherapy as first-line LLT (Table). Treatment gaps of >3 months in first-line were observed in 12.5% of patients. Per patient, a mean (median) of 1.6 (1) treatment gaps was observed with a median length of 208 days. Most treatment gaps lasted for 3 to 6 months (44.7%), whereas longer gaps were observed less frequently with 24.3% and 31.0% for treatment gaps of 6 to 12 or >12 months, respectively. Permanent treatment discontinuation was observed in <5% of patients.
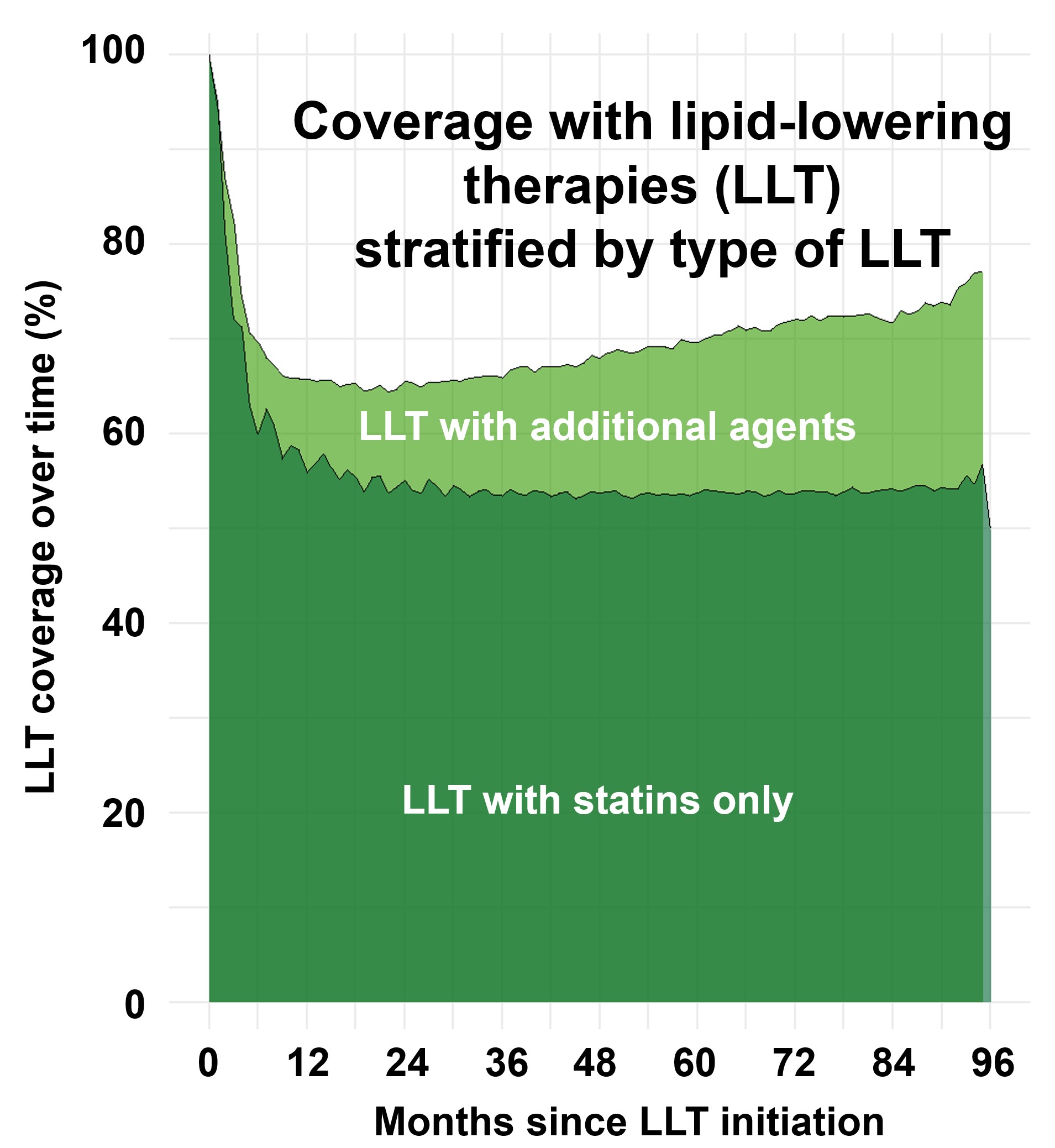
The LLT coverage showed a steep decline in the first 12 months after index LLT prescription, and remained stable at 55% to 60% in the further treatment course (Fig. 1). Patients with a more recent date of LLT initiation showed a trend towards higher LLT coverage within the first year of treatment (Fig. 2). Finally, LLT regimens only containing a statin had lower LLT coverage than those containing non-statin LLT (Fig. 3).
ConclusionsGaps in LLT of >3 months were observed in 12.5% of patients with at least two LLT prescriptions. The LLT coverage of 55-60% indicates that on average, utilisation of LLT is better than expected based on previously reported long-term persistence rates of 20-30%, however with still room for improvement. Treatment coverage with LLT may serve as an additional marker to estimate the expected benefits of LLT at the population level.
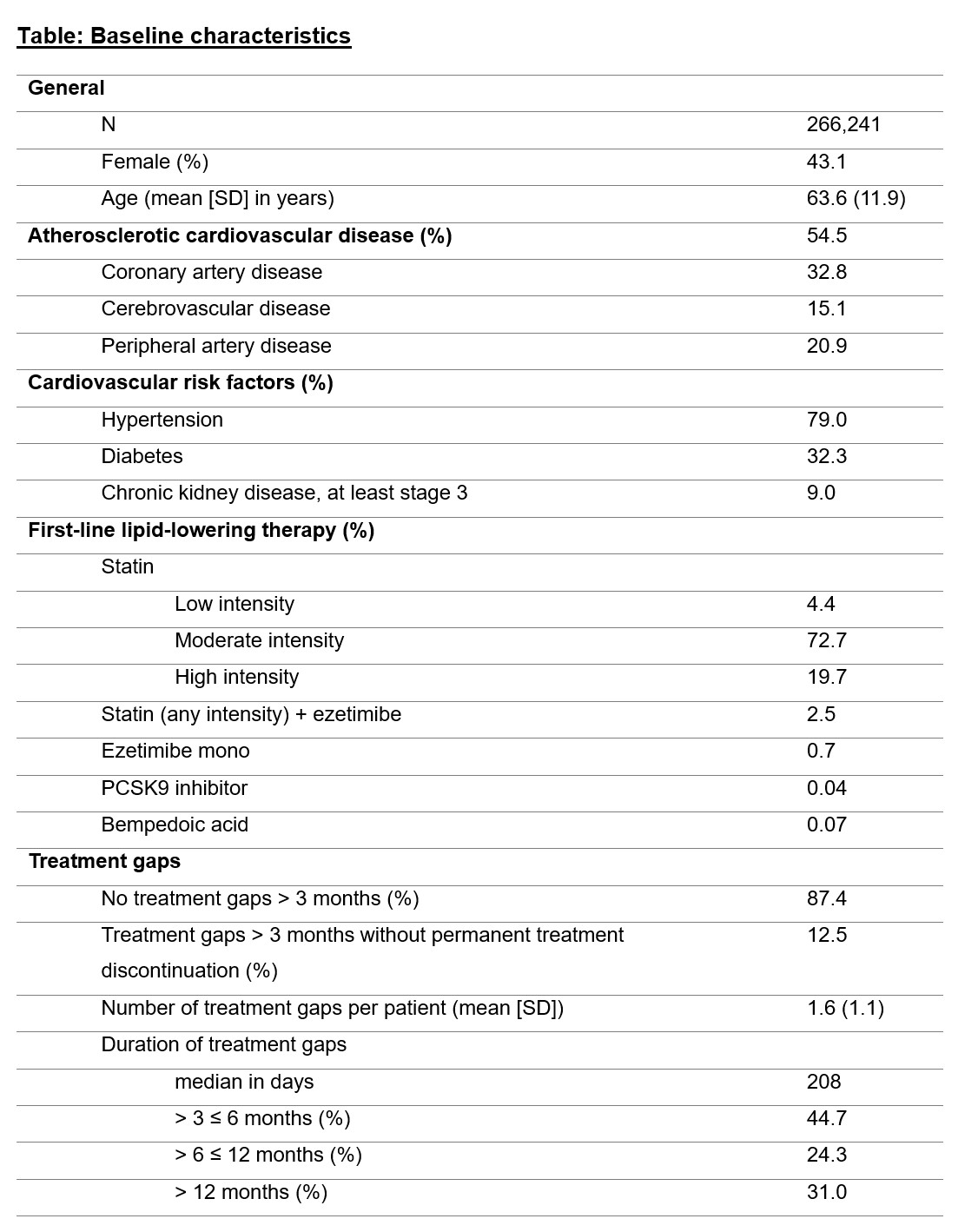
Fig. 1
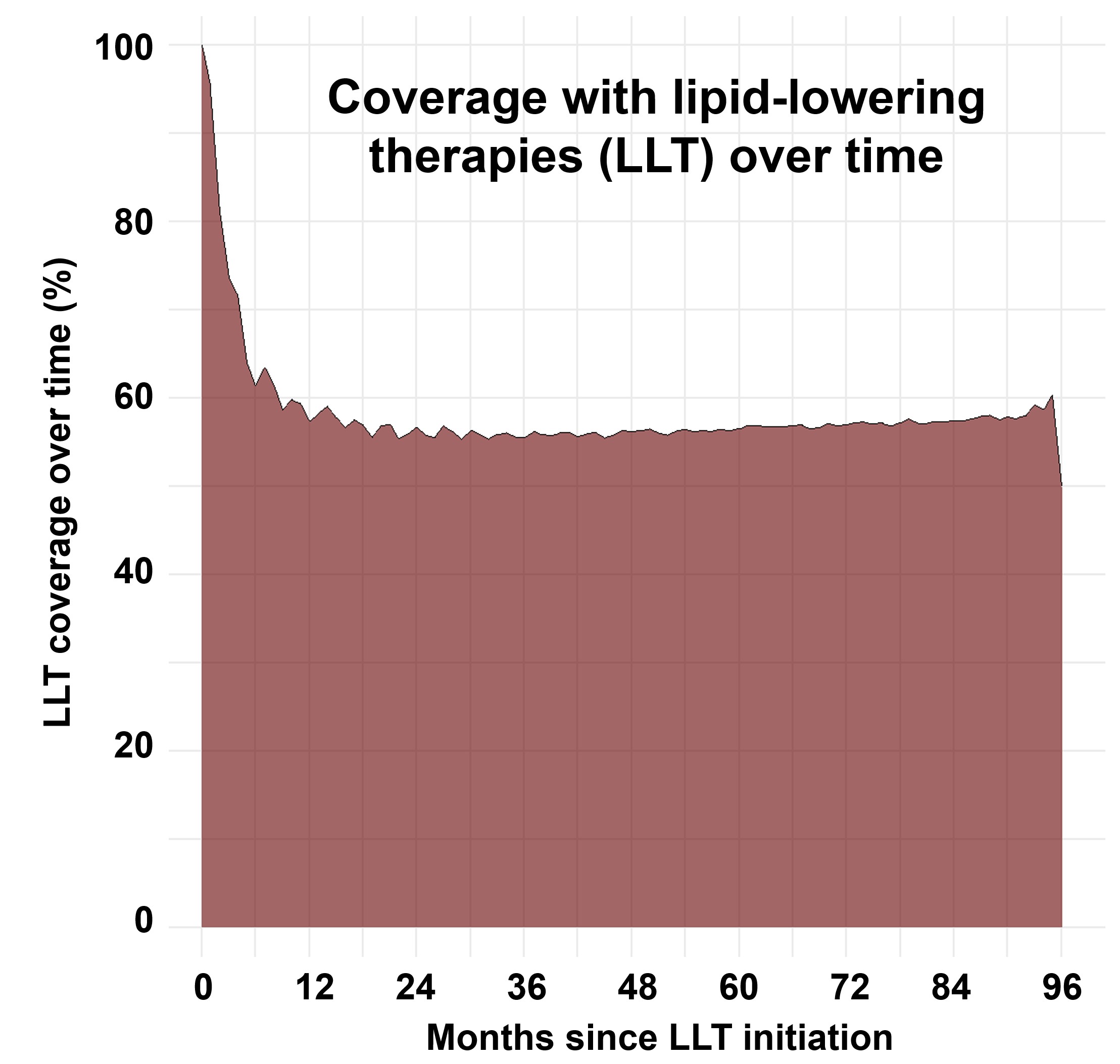
Fig. 2
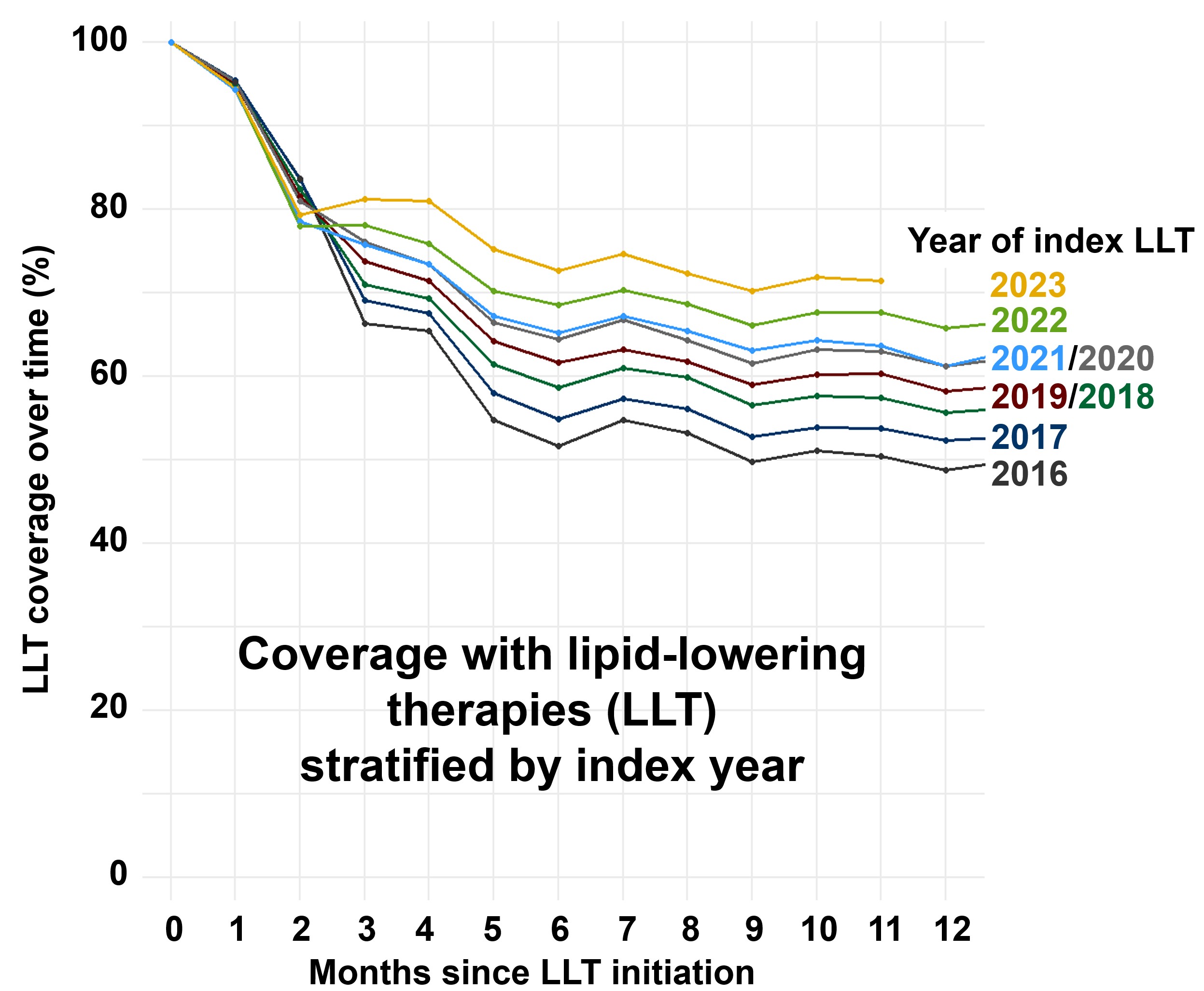
Fig.3