Background
Third-degree atrioventricular block (AVB) remains the most common complication following transcatheter aortic valve replacement (TAVR) requiring permanent pacemaker implantation (PPI). Current guidelines recommend an observation period of at least 48 hours. Pre-existing right bundle branch block (BBB) and dynamic prolongation of the PQ interval have been identified as predictors of developing high-grade/complete AVB.
The aim of the study was to evaluate the ventricular pacing burden (VP) post TAVR to better understand the natural course of conduction disorder and to identify potential influencing factors.
Methods
This single-center retrospective cohort study includes all consecutive patients who received a PPI due to AVB following TAVR from 09/22 to 08/25. Electrocardiograms were obtained before and after TAVR, as well as pacemaker data after implantation and during follow-up (FU) after seven weeks. For each patient, ΔVP between time of TAVR and FU was assessed as a marker for AVB dynamic.
Results
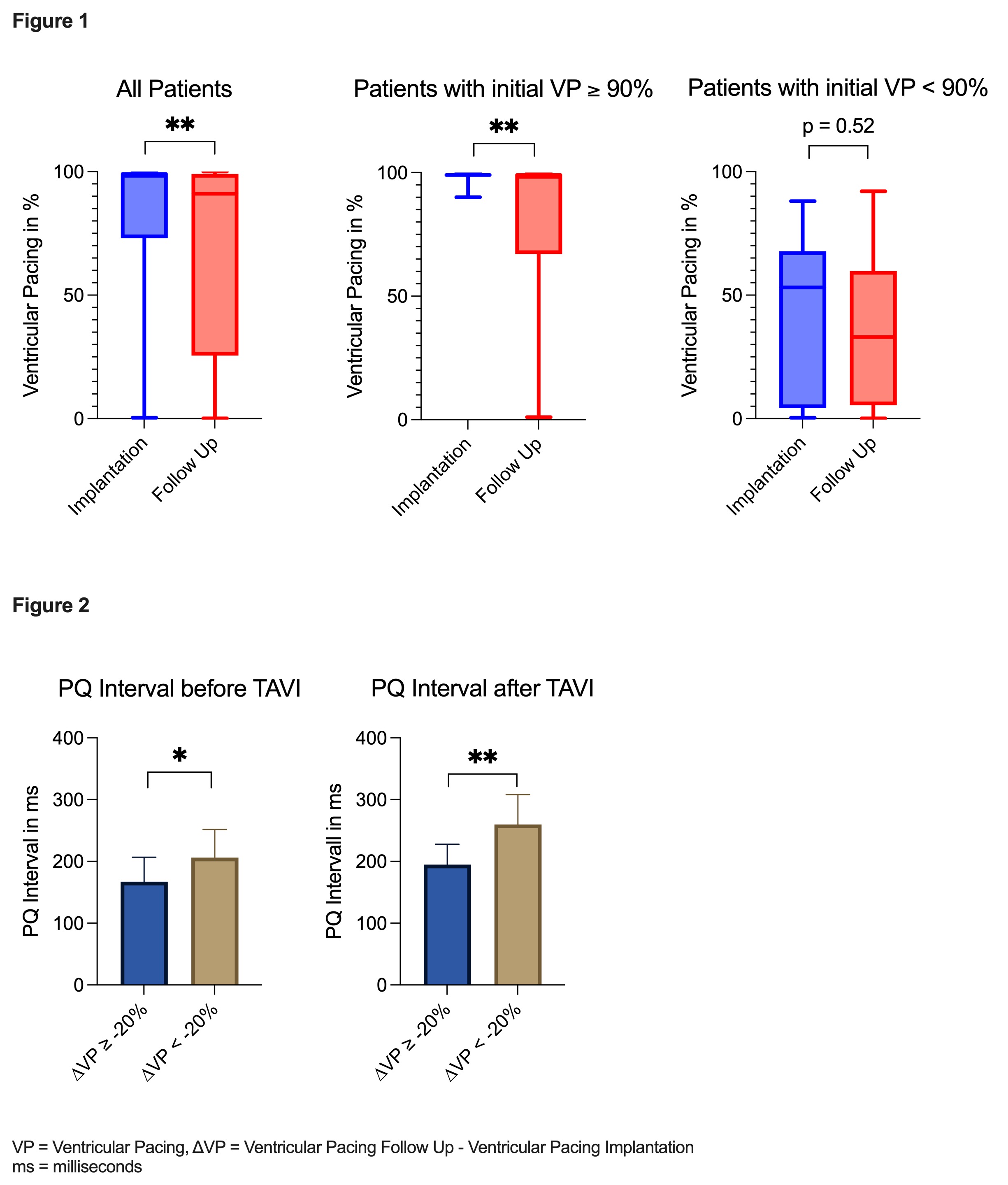
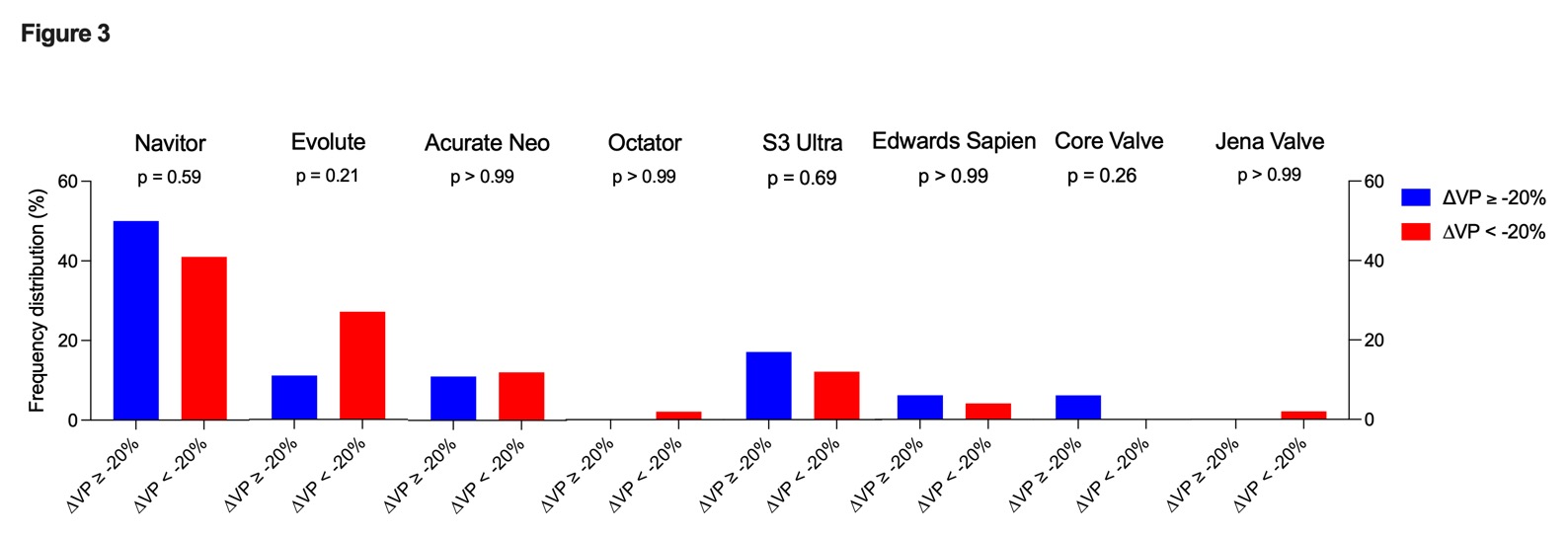
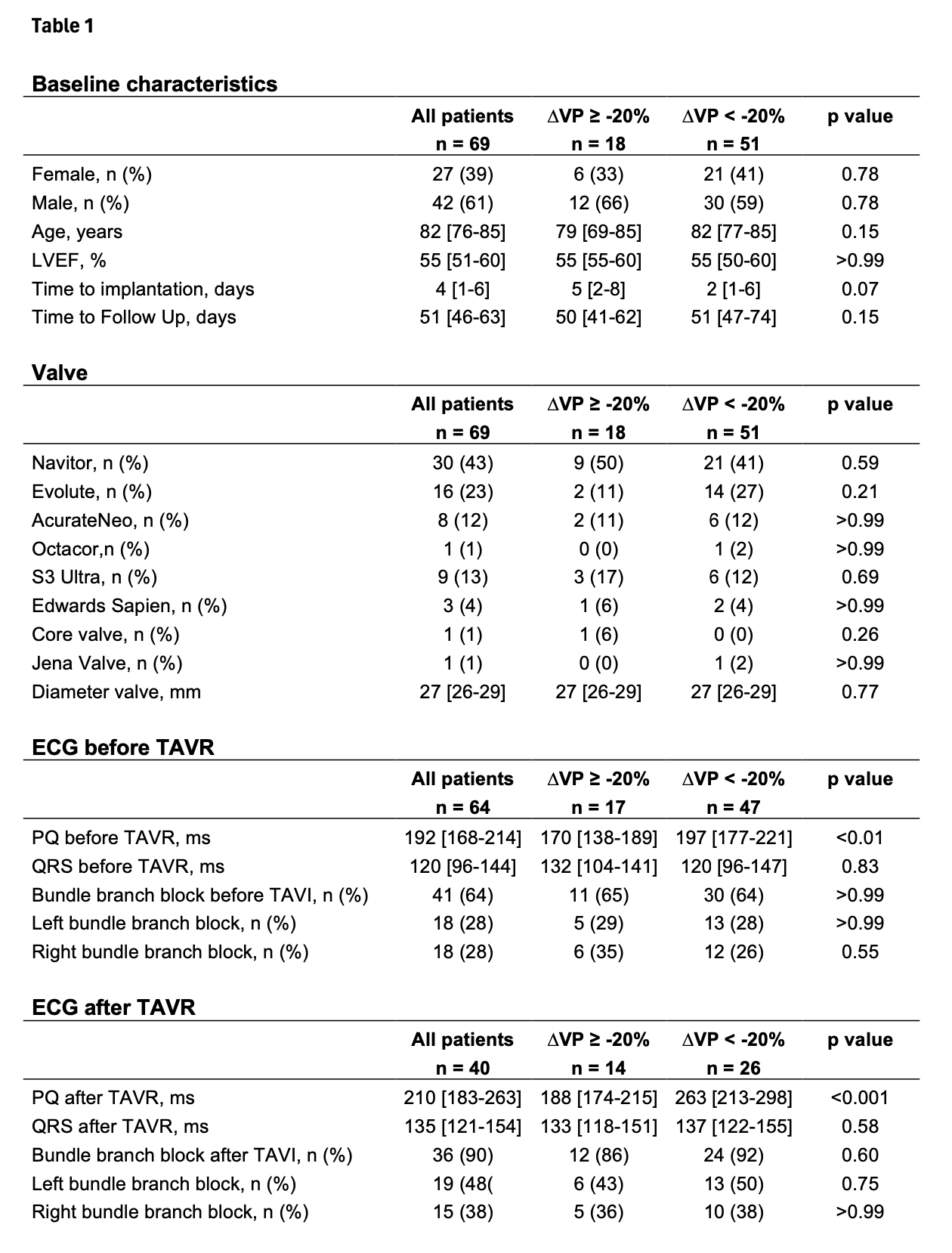
A total of 69 patients underwent PPI and were analyzed: 39% were female, median age was 82 years. No differences were observed in baseline characteristics (table 1). The VP showed a significant reduction during FU (99% vs. 91%, p<0.01; fig. 1). Our subgroup analysis including only patients with VP≥ 90% at baseline showed a significant reduction in VP (p<0.01), whereas patients with initial VP<90% showed no significant VP dynamic (fig. 1). After ΔVP stratification, the group with ΔVP of at least -20% had a significantly shorter PQ interval on the pre-TAVR ECG vs. patients with ΔVP less than -20% (170ms vs. 197ms; p<0.01; Fig. 2). In line with these results also a shorter PQ interval after TAVR was observed in patients ΔVP of at ≥-20% vs. <-20% (188ms vs. 263ms; p<0.001, Fig. 2). In contrast, QRS width and BBB pre/post TAVR were not associated with ΔVP changes. Furthermore, no significant differences were observed with respect to TAVR type and diameter used (Fig. 3).
Conclusion
Our study demonstrated a dynamic change in VP post TAVR. Patients with initially high VP showed a significant VP reduction over time. A shorter PQ interval was associated with increased VP dynamics, while QRS width and preexisting BBB were not significant predictors. Our results provide novel insights into the role of PQ interval being more relevant than QRS variables for prediction of future VP burden and VP dynamics, independent of TAVR type used.