Background: Electrocardiographic (ECG) findings such as sinus tachycardia and right bundle branch block are commonly associated with acute pulmonary embolism (PE).
Objective: This study aimed to investigate the prevalence of advanced interatrial block (IAB) in patients with acute PE and its association with atrial fibrillation (AF) and hemodynamic changes.
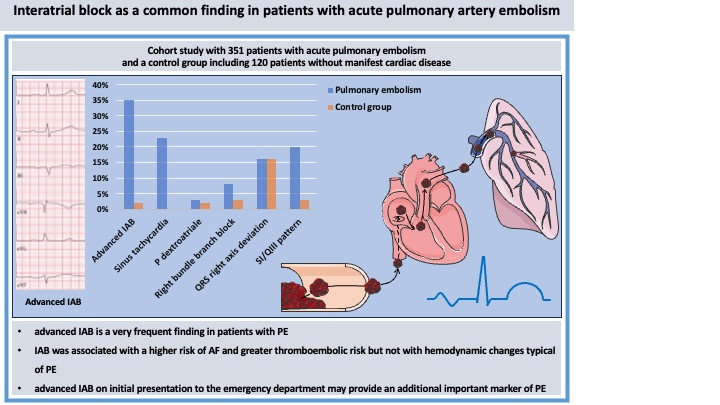
Methods: This cohort study included patients diagnosed with acute PE between January 2014 and September 2024 at University Hospital Münster. A control group of individuals without manifest heart disease served as a control group. All patients underwent clinical, laboratory, ECG, and echocardiographic evaluations.
Results: A total of 351 patients with acute PE and 120 control patients were included. The PE group had a mean age of 62.5 years. Advanced IAB was detected in 35% of PE patients, significantly higher than in controls (2%). In contrast, typical ECG signs of PE such as sinus tachycardia (23%), right bundle branch block (8%), and S1Q3 pattern (20%) were less frequent. A subgroup analysis demonstrated that patients with IAB were older, had a higher CHA2DS2-VA score, and were more likely to have pre-existing and new-onset AF. IAB was not associated with right heart dysfunction on echocardiography.
Conclusion: For the first time, this study revealed that advanced IAB was present in many patients with acute PE. IAB was associated with a higher risk of AF and greater thromboembolic risk but not with hemodynamic changes typical of PE. Detecting an advanced IAB at the initial presentation in the emergency department could provide an important indication of PE.