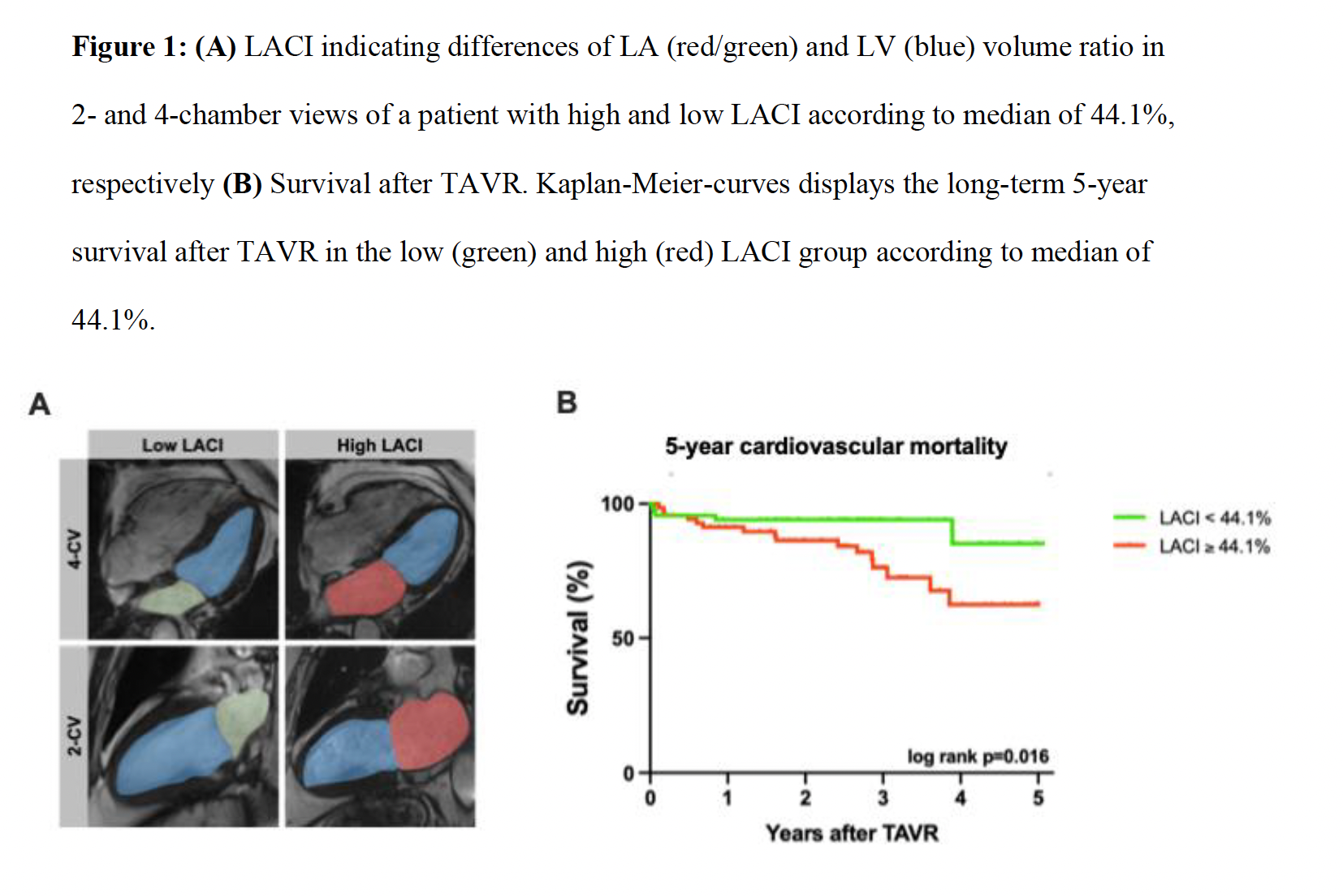
Background: Transcatheter aortic valve replacement (TAVR) is a well-established therapy for severe aortic stenosis (AS), with procedural volumes continuing to rise. Precise risk stratification is essential to optimize patient selection and to improve patient monitoring beyond procedural success. Cardiovascular magnetic resonance (CMR)–derived left atrioventricular coupling index (LACI) is a novel and easy measurable imaging marker, capturing the structural relationship between the left atrial (LA) and left ventricle (LV). Whether CMR-derived LACI possesses and adds prognostic value beyond established outcome predictors in patients with severe AS remains unknown. We therefore hypothesized that CMR-derived LACI can predict adverse outcomes in patients with severe AS undergoing TAVR. Methods: Patients with severe symptomatic AS referred for TAVR were prospectively included and underwent pre-procedural CMR between January 2017 and March 2023. LACI was defined as the ratio of the indexed LA end-diastolic volume (LAEDVi) to indexed LV end-diastolic volume (LVEDVi) (Figure 1A). The primary clinical endpoint of this study was cardiovascular (CV) mortality during 5-year follow-up. The cohort was dichotomized into groups with high and low LACI according to median. Groups were compared using the Mann–Whitney U and Chi-square test. Associations with CV mortality were assessed by univariable and multivariable Cox proportional-hazards models adjusted for relevant clinical and imaging covariates. Furthermore, survival was compared using Kaplan–Meier estimates and log-rank testing. Results: In total 138 patients (80y [75 – 83], 62.3% male) were included in final study analyses. Patients with high LACI according to median (≥44.1%) were at higher NYHA III–IV class (68.1% vs 44.9%; p=0.047), had a greater prevalence of atrial fibrillation (50.7% vs 14.5%; p<0.0001) and elevated NT-proBNP (2017ng/L vs 1012ng/L; p=0.007). On CMR, LV ejection fraction (LVEF) and LV global longitudinal strain (LV GLS) did not differ significantly between both groups. However, patients with high LACI showed an impaired RV function (RVEF 49.1% vs 55.9%; p=0.003; RV GLS −25.1% vs −28.7%; p=0.015) and lower biatrial strain values (LA Es 9.7% vs. 16.3%; p<0.001, RA Es 13.9% vs. 16.5%; p=0.028). LACI was significantly associated with CV mortality (HR 3.92, 95% CI 1.18–15.97; p=0.014) and over a median follow-up of 2.7 years (IQR 1.7–3.6), patients with high LACI values showed worse survival compared to those with low LACI (log-rank: p=0.016, Figure 1B). In multivariable Cox regression models, LACI remained independently associated with CV mortality after adjustment for established parameters of myocardial function, including LVEF and LV GLS (LVEF: HR 2.33, 95% CI 1.10–4.90; p=0.026, LV GLS: HR 2.21 95% CI 1.00 – 4.9, p=0.049). Conclusion: CMR-derived LACI is associated with CV mortality in patients with severe symptomatic AS undergoing TAVR. LACI assessment offers independent prognostic value and facilitates additional risk stratification, while its simple and rapid calculation allows easy integration into clinical routine for optimized patient management.