Background: Due to the high coincidence of atrial fibrillation (AF) and coronary artery disease (CAD), feasibility and safety of concomitant rhythm control and percutaneous coronary intervention (PCI) need to be evaluated.
Methods: Consecutive patients who received concomitant rhythm control for AF (catheter ablation [CA-AF] and/or electric cardioversion [ECV]) and PCI for CAD (drug eluting stent implantation) within the same hospital stay between 2017 and 2024 were retrospectively analyzed for acute in-hospital complications (death, cardiogenic shock, sepsis, pericardial tamponade, thromboembolic events, major bleedings, pacemaker implantation, and coronary artery dissection). Post-discharge adverse event rates and AF-recurrence freedom were evaluated by assessing subsequent hospital stays and conducting a structured telephone follow-up. Results were stratified by admission status (emergency vs. elective) and type of rhythm control (CA-AF vs. ECV only).
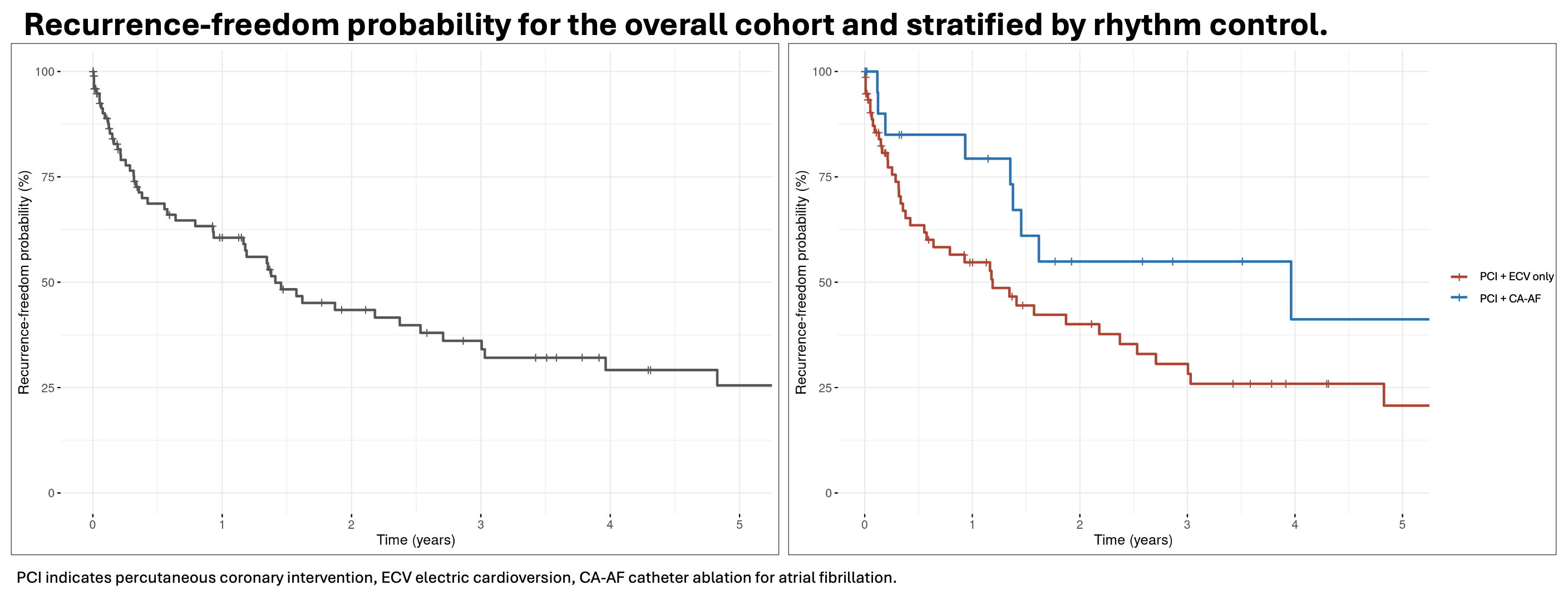
Results: In total, 115 patients received concomitant rhythm control for AF and PCI for CAD (77% male, mean age 74±8 years). CA-AF was performed in 23% of the patients. PCI for acute myocardial infarction (MI) was indicated in 34 patients (30%). Overall, in-hospital complication rate was 11%. 81 patients (70%) were admitted via the emergency department and 34 patients (30%) were admitted electively. There were no significant differences in age, sex, and comorbidities between elective patients and emergency patients, however, elective patients more frequently underwent CA-AF (41% vs. 16%, p=0.004). There were no differences in the rates of acute in-hospital complications between emergency patients and elective patients (11% vs. 12%, p>0.99). Patients who underwent PCI and CA-AF (23%) had in comparison to patients who received PCI and ECV only (77%) more often paroxysmal AF (19% vs. 1.1%, p=0.003), while age, sex and comorbidities were similar. Patients undergoing two invasive procedures (PCI and CA-AF) had in comparison to patients undergoing PCI and ECV only non-significant lower complication rates (7.4% vs. 13%, p=0.73) and similar bleeding rates as (3.7% vs. 3.4%, p=0.17). Overall, the 12-months adverse event rate was 18.8% (mortality 3.5%, major bleeding 5.9%, hemorrhagic stroke 1.2%, pacemaker implantation 2.4%, MI 5.9%), however, no thromboembolic events occurred. The probability of freedom from AF-recurrence at 1 year was 60.6%. Patients who underwent CA-AF had a higher probability for freedom from AF-recurrence compared to patients receiving ECV only (79.3% vs. 54.7%).
Conclusion: Potentially life-threatening procedure-related complications such as major bleedings and thromboembolic events are rare in patients undergoing concomitant rhythm control for AF and PCI for CAD, even if two invasive procedures are performed. However, 12-months adverse event rates were at 18.8% due to the patients’ underlying multi-morbidity and combined anticoagulation strategies with potentially increased bleeding risk. Notably, patients who received CA-AF had a higher probability of remaining free of AF without an increase in acute in-hospital complications.