Background: Multiple attempts of grasping are routinely necessary during mitral valve transcatheter-edge-to-edge repairs (M-TEER) to optimize residual mitral regurgitation (MR). Whether an increased number of grasping attempts using the PASCAL device is associated with higher risk of leaflet injury, leading to worse procedural outcomes remains unknown.
Objectives: We evaluated safety, procedural characteristics and sustainability of MR reduction in procedures with low vs. high number of grasping attempts during M-TEER with the PASCAL system.
Methods: We retrospectively evaluated consecutive patients with severe MR who underwent M-TEER between 2019 and 2024 at our center using the PASCAL or PASCAL ACE system. Grasping attempts were classified into two groups: ≤80
th percentile of grasping attempts (≤7 grasping attempts) vs. >80
th percentile (≥8 grasping attempts). Baseline, procedural, short- and mid-term characteristics as well as sustainability of residual MR was compared between groups.
Results: Overall, data from 391 procedures (77.7 ± 10.1 years, 57.5% male) were evaluated in our analysis. In the group of procedures with low number of grasping attempts, a median of 4 (2; 5) grasping attempts were performed. In contrast, 10 (9; 12; max. 22) grasping attempts were performed in the group of above 80
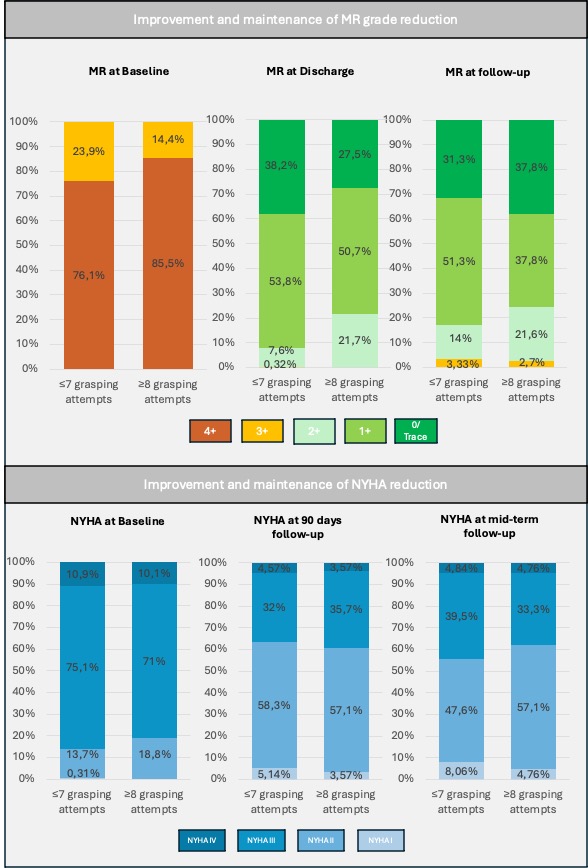
th percentile of grasping attempts. No single leaflet detachment, leaflet injury or any other device-related complication was observed in any of the groups. Procedure length was significantly higher in patients and with ≥8 grasping attempts (126 ± 47.6 vs. 82.9 ± 43.3 minutes, p<0.001). Patients with ≥8 grasping attempts had higher EROA at baseline (0.48 cm² [0.38; 0.70] vs. 0.40 cm² [0.30; 0.50], p=0.00036). Interestingly, complexity criteria were not more frequently present in cases with many grasping attempts: ≥2 independent Jets: 17.4% vs. 16.8%; p=1, mitral valve orifice area <4 cm²: 37.9% vs. 40.8%; p=0.76, significant Jet in the commissural area: 21.7% vs. 16.5%; p=0.38, flail width >15mm and/or flail gap >10mm: 10.1% vs. 8.39%, p=0.81, others: 18.8% vs. 15.2%; p=0.57). Improvement in MR severity from baseline to discharge, as well as sustainability of residual MR from discharge to mid-term follow-up (434 [176; 699] days after the procedure) were not different between groups with high vs. low number of grasping attempts (p=0.11 for differences in MR improvement from baseline to discharge, p=0.09 for sustainability of MR reduction from discharge to mid-term follow-up, Figure). Likewise, NYHA functional class improvement was similar between groups (p=0.99 for differences in improvement from baseline to 90 days, p=0.78 from baseline to mid-term follow-up). Also, the overall mortality was not different for procedures with ≥8 vs. ≤7 grasping attempts (7.25% vs. 6.52%, p=1).
Conclusion: Using the PASCAL system, multiple procedural grasping attempts during M-TEER are safe and result in comparable MR reduction, sustainability and mid-term outcomes as compared to procedures with fewer grasping attempts. Our results support the routine use of multiple grasping attempts in M-TEER procedures if procedural results are suboptimal after initial attempts.