Introduction: Pulsed-field ablation (PFA) has emerged as an alternative energy source for pulmonary vein isolation (PVI) in atrial fibrillation (AF). Long-term data on efficacy and clinical outcomes remain limited. This study aimed to investigate differences in procedural characteristics, safety and clinical outcomes between patients undergoing PFA and cryoballoon ablation (CBA).
Methods: A prospective, observational, single-center study was conducted, enrolling patients with symptomatic AF undergoing initial PVI using either CBA or PFA. To enhance the statistical robustness of the comparison, propensity score 2:1 matching was performed based on six baseline parameters: sex, age, body mass index (BMI), left atrial diameter, AF type, and mitral regurgitation. Subsequently, procedural and safety data, as well as clinical outcomes, were compared between the two groups.
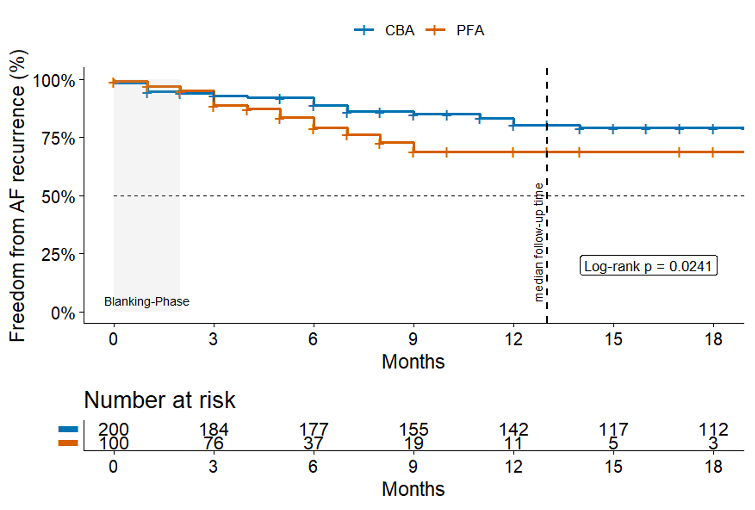
Results: Between May 2012 and August 2025, a total of 2,164 patients underwent initial PVI by means of CBA or PFA. The final study cohort included 100 patients treated with PFA and 200 propensity-matched patients treated with CBA. Matching analysis demonstrated excellent covariate balance (SMD < 0.1). The mean age was 64.5 ± 13.2 years, and 39.0% were female. The mean LA diameter was 39.6 ± 7.3 mm, and the mean BMI was 26.1 ± 4.7 kg/m². Moderate or severe MR was present in 9 (3%) patients. No significant differences were observed in baseline characteristics between groups. Acute PVI was achieved in all patients (100%).A total of 15 complications occurred across both groups, with no cases of MACCE. Three (1.0%) major complications were reported in the CBA group, including two (0.7%) persistent phrenic nerve palsies and one (0.3%) groin complication requiring surgical intervention. No major complications occurred in the PFA group. Minor complications were observed in 9 (4.5%) CBA patients and 3 (3.0%) PFA patients. No significant differences were found in overall safety outcomes.During a median follow-up of 13 months [IQR 24.2], 80 (26.7%) patients experienced AF recurrence. However, follow-up duration differed significantly between groups (5 months for PFA vs. 21 months for CBA; p < 0.001). Outcome analysis revealed a higher rate of AF recurrence in the PFA group compared with the CBA group (p = 0.024). The corresponding Kaplan–Meier analysis is shown below. More CBA patients were on anti-arrhythmic drugs of class I/III (AAD) at hospital discharge (14.5% vs. 4%, p=0.006). AAD rate at follow-up was not different between groups (4% vs. 3%, p=0.757).
Conclusion: In this propensity score–matched analysis, both CBA and PFA demonstrated excellent acute efficacy and a favorable safety profile for initial PVI in patients with AF. No major complications occurred in the PFA group. Follow-up data shows that AF recurrence is slightly higher in PFA. PFA appears to be a safe and effective ablation modality, warranting further evaluation in larger cohorts with extended follow-up to confirm its long-term efficacy relative to established thermal techniques.