Background:
Extracorporeal cardiopulmonary resuscitation (ECPR) offers a potential life-saving intervention in refractory cardiac arrest. While shorter low-flow time (LFT) is generally associated with improved outcomes, evidence regarding ECPR effectiveness beyond the often-cited 60-minute threshold remains limited. This study aimed to assess nearly a decade of single-center experience with ECPR in patients with prolonged LFT over 60 minutes and to identify factors associated with survival in this high-risk population.
Methods:
This retrospective, single-center study included 268 consecutive patients who underwent ECPR for refractory cardiac arrest with a cumulative LFT ≥60 minutes. LFT was defined as the time from emergency call or arrest in the ambulance to ECMO initiation. Patients with implausible or extreme timing parameters were excluded: no-flow time >20 min (n=5), alarm-to-ACLS >30 min (n=1), door-to-ECMO >60 min (n=16), and insufficient baseline data (n=11), resulting in 235 patients for final analysis. Logistic regression models were used to associate low flow time and other covariables with overall survival to discharge. The graphical representation was done with log odds plots.
Results:
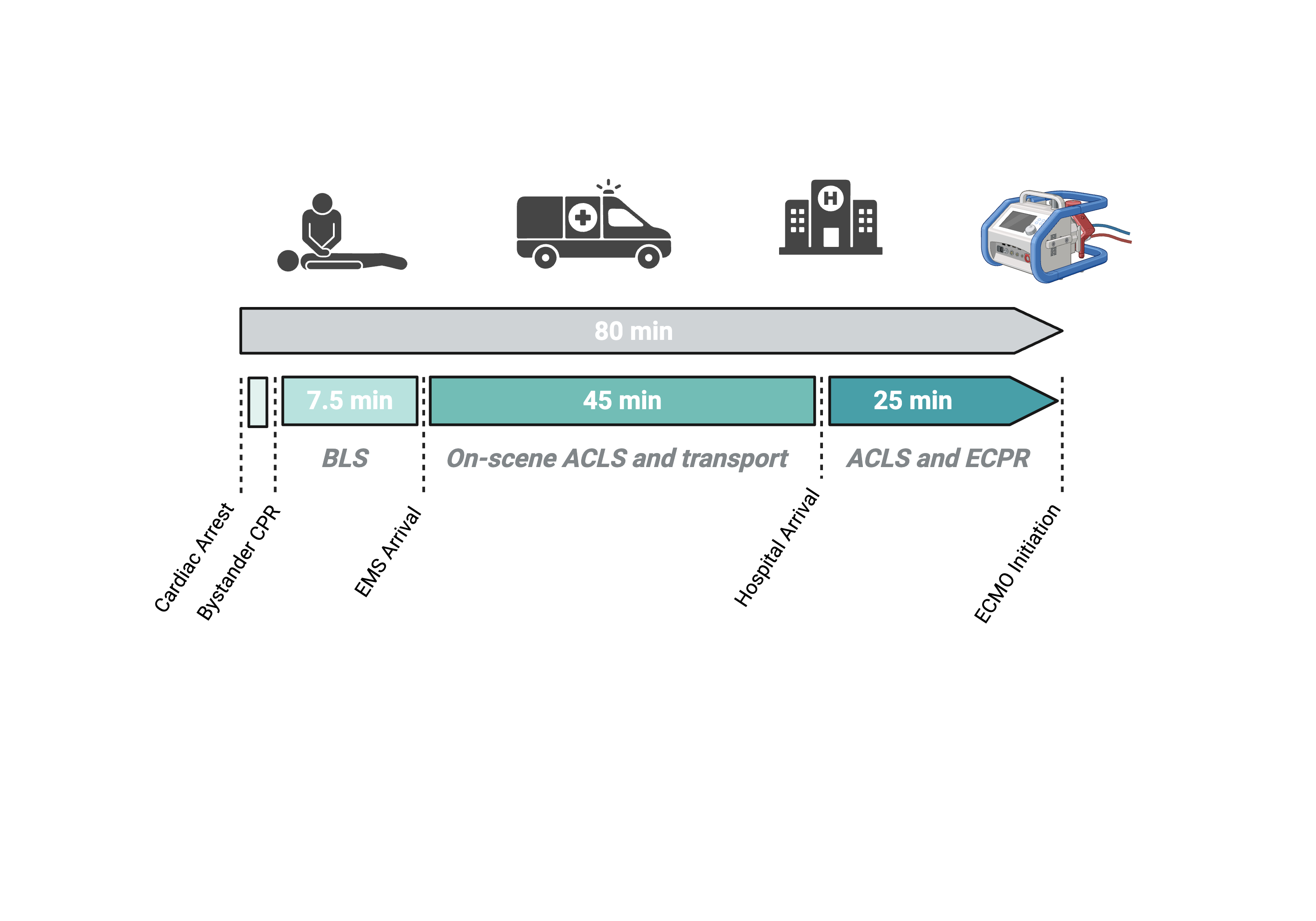
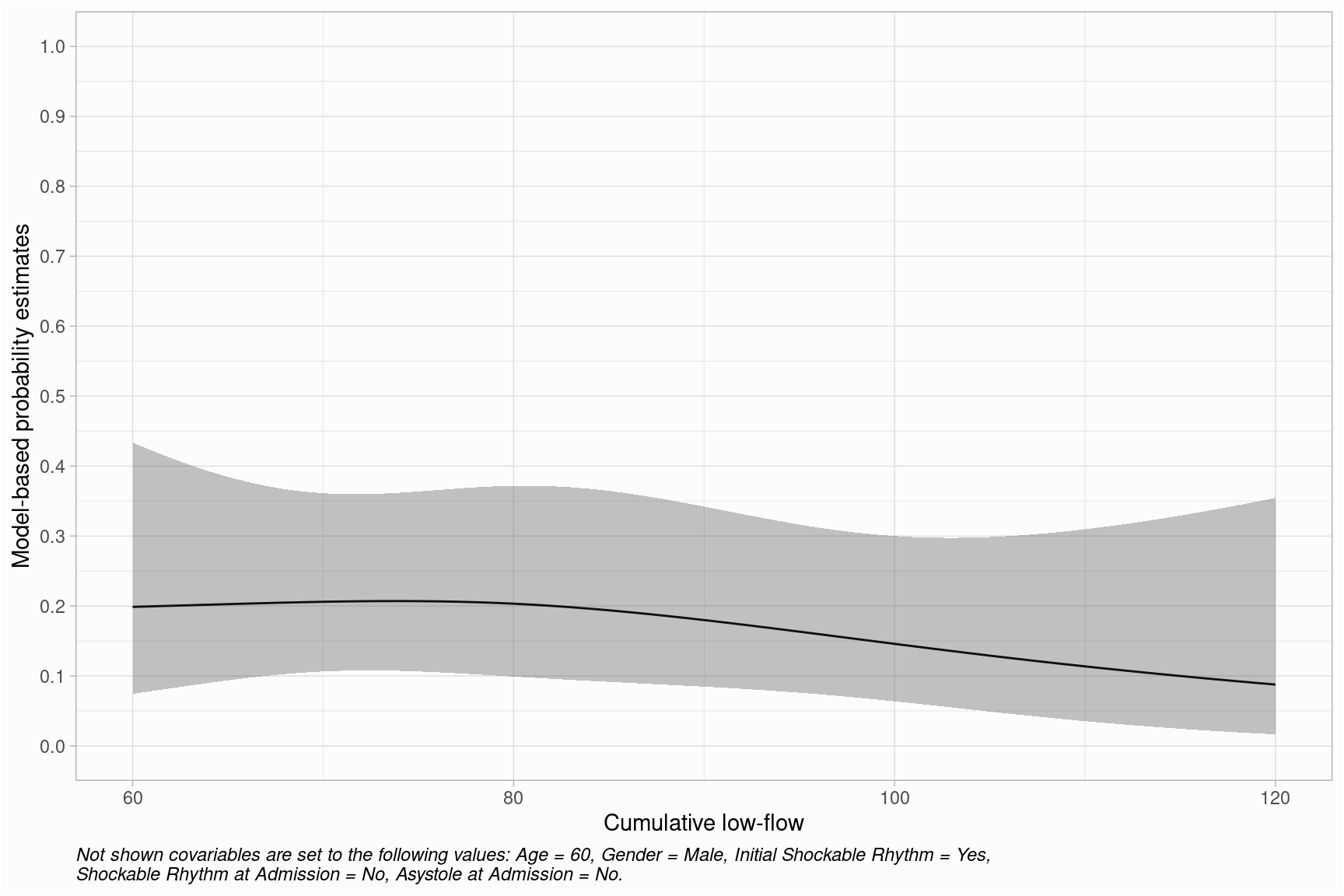
Overall survival to hospital discharge was 16.1% (n=38). Of those, 79% (n=30) achieved favorable neurological outcomes defined as £2 in the cerebral performance category scale. The median cumulative LFT was 80 minutes. Key resuscitation median time intervals were: 7.5 minutes to ACLS initiation, 45 minutes of transport time, and 25 minutes of in-hospital resuscitation before ECMO initiation (Figure 1). The longest LFT among survivors was 115 minutes, and 100 minutes among those with favorable neurological outcome. Survival with LFT of more than 90 minutes was rare (n = 6), which was consistent with the estimated, model-based probability of survival. This showed that, after the initial plateau, the probability of survival decreased gradually after 80 minutes (Figure 2).
Survivors showed higher rates of cardiac cause (82 vs. 63%), witnessed arrest (92.1 vs. 85.3%), direct ACLS (26 vs. 17%) and bystander CPR (86.8% vs. 82.2%), as well as more favorable biochemical parameters on admission: lower lactate (12.3 vs. 14.5 mmol/L), lower pCO₂ (68 vs. 71 mmHg), and higher pH (7.00 vs. 6.91). Logistic regression models identified female gender, intermittent return of spontaneous circulation, an initial shockable rhythm, a shockable rhythm and absence of asystole upon hospital arrival as independent positive prognostic factors.
Conclusion:
Although survival rates decline with increasing low-flow time, ECPR may still offer a survival benefit even beyond 60 minutes of LFT in selected patients. The routine use in this population should be carefully evaluated. The presence of sustained electrical activity, particularly shockable rhythms, and intermittent ROSC may help to guide patient selection, particularly since biochemical parameters seem to have no clinical relevance. Further optimization of pre- and in-hospital management is needed to improve outcomes in prolonged resuscitation scenarios.