Background
Periodic repolarization dynamics (PRD) is a novel ECG-derived biomarker reflecting sympathetic activity–associated oscillations in cardiac repolarization. We hypothesized that elevated PRD identifies patients after acute ischemic stroke (AIS) who are at increased risk of developing atrial fibrillation detected after stroke (AFDAS).
Methods
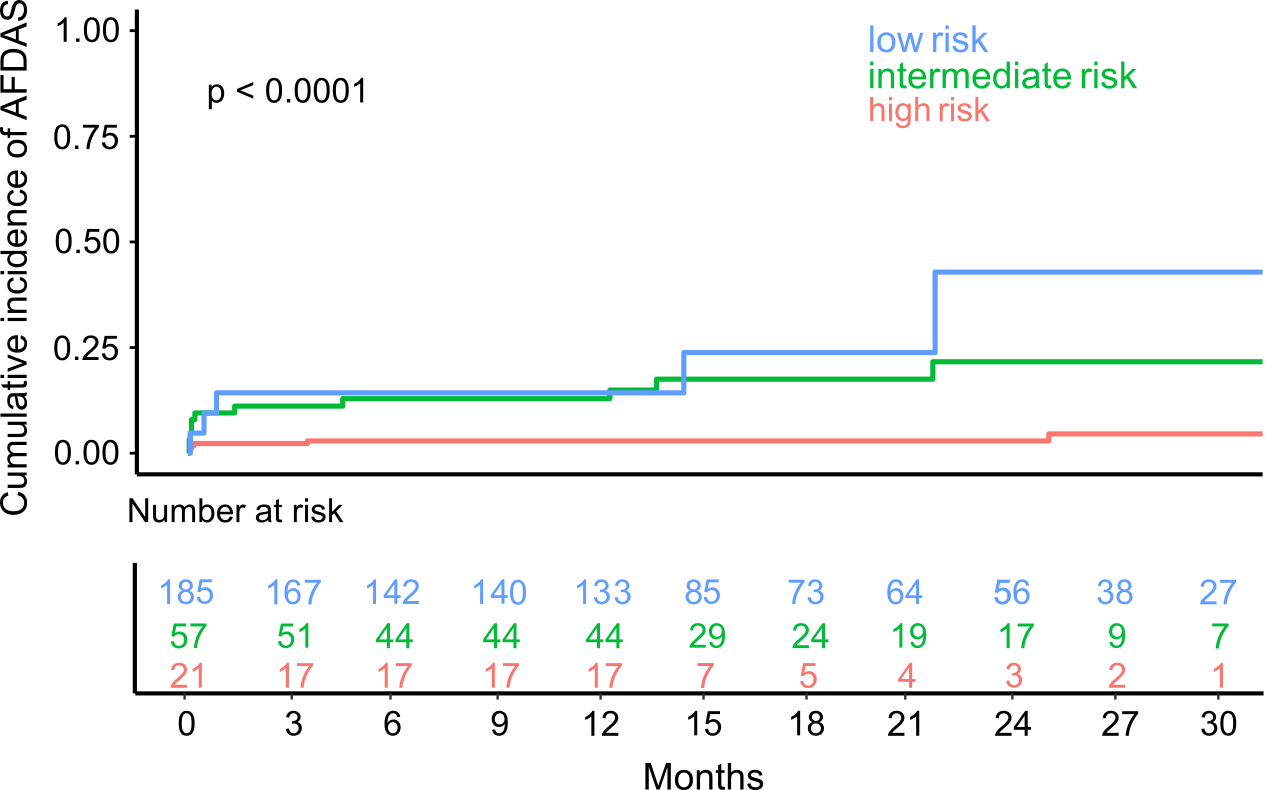
Between February 22, 2021, and May 5, 2023, 263 patients with AIS from the STROKE-CARD II cohort were prospectively enrolled. All patients were in sinus rhythm at baseline without prior or current atrial fibrillation (AF). Within 5 days after AIS, patients underwent a standardized 30-minute high-resolution ECG to assess PRD, heart rate variability, and supraventricular premature complexes (SPCs/hour). AFDAS was identified through continuous in-hospital monitoring, 6-month follow-ups, and electronic health record review. The CHASE-LESS score served as the clinical risk model for AFDAS. Based on dichotomized PRD and SPC frequency, three risk categories were defined: low risk (both normal; n = 185), intermediate risk (PRD or SPC frequency abnormal; n = 57), and high risk (both abnormal; n = 21).
Results
During a median follow-up of 19 (IQR 14) months, AFDAS occurred in 25 of 263 patients (9.5%). Patients with AFDAS exhibited higher PRD values than those without (5.80 vs. 2.93 deg², p = 0.005). In multivariable Cox regression, PRD independently predicted AFDAS (HR 1.27, 95% CI 1.03–1.44, p = 0.037), alongside SPC frequency (HR 1.02, 95% CI 1.01–1.03, p < 0.001). A model comprising PRD and SPC per hour showed better discrimination than the CHASE-LESS score alone, with an AUC of 0.82 versus 0.67 respectively (p = 0.005). AFDAS prevalence markedly differed across the risk groups: 6/21 patients (28.6%) exhibited AFDAS in the high-risk group, 10/57 (17.5%) in the intermediate-risk group, and 4/185 (2.1%) in the low-risk group (p < 0.001). Compared to the low-risk group, patients in the high-risk and intermediate-risk groups had an 11.3-fold (95% CI 3.6–35.8) and 6.7-fold (95% CI 2.5–17.7) increased risk of developing AFDAS (p < 0.001 for both). The negative predictive value of the low-risk group was 97.9%, and the positive predictive value of the high-risk group was 28.6%.
Conclusions
Increased PRD and SPC frequency independently predict AFDAS and significantly improve risk prediction compared to the clinical CHASE-LESS score.