Background: Cardiovascular diseases (CVD) remain a leading cause of morbidity and mortality worldwide. Low-dose antiplatelet therapy with acetylsalicylic acid (ASA) is recommended for persons with established CVD, while there is no evidence supporting ASA intake in primary prevention. We investigated the prevalence, patterns, and predictors of ASA intake in primary and secondary prevention using population-based data.
Methods: Data from 203,413 participants of the German National Cohort Study (NAKO) were analyzed. Regular ASA intake was assessed using ATC codes and compared with no regular intake. Participants were stratified by prevalent CVD status (primary vs. secondary prevention). Sociodemographic factors, comorbidities, and concomitant cardiovascular medication were assessed. Predictors of ASA intake were identified using multivariable logistic regression adjusted for age, sex, and established cardiovascular risk factors.
Results: 11,008 persons (5.4%) reported regular ASA use. Among ASA users, 59.6% also reported CVD and thus used ASA for secondary prevention. Among participants with CVD (n=12,062), 53.2% reported ASA use and 66% any form of antiplatelet or anticoagulant therapy, leaving 34% untreated. In multivariable analysis, prevalent CVD was the strongest predictor of ASA intake, including stroke (OR 15.44, 95% CI 14.06, 16.94), myocardial infarction (OR 11.75, 95% CI 10.53, 13.12), and peripheral artery disease (OR 3.82, 95% CI 3.46, 4.22), respectively. Female sex was inversely associated with ASA intake (OR 0.62, 95% CI 0.59, 0.65).
Conclusion: In this large population-based cohort, only half of persons with prevalent CVD reported regular ASA intake, leaving a substantial proportion untreated. Prior myocardial infarction and stroke were the strongest predictors of ASA use, while women were less likely to receive ASA. These findings highlight important gaps in secondary prevention.
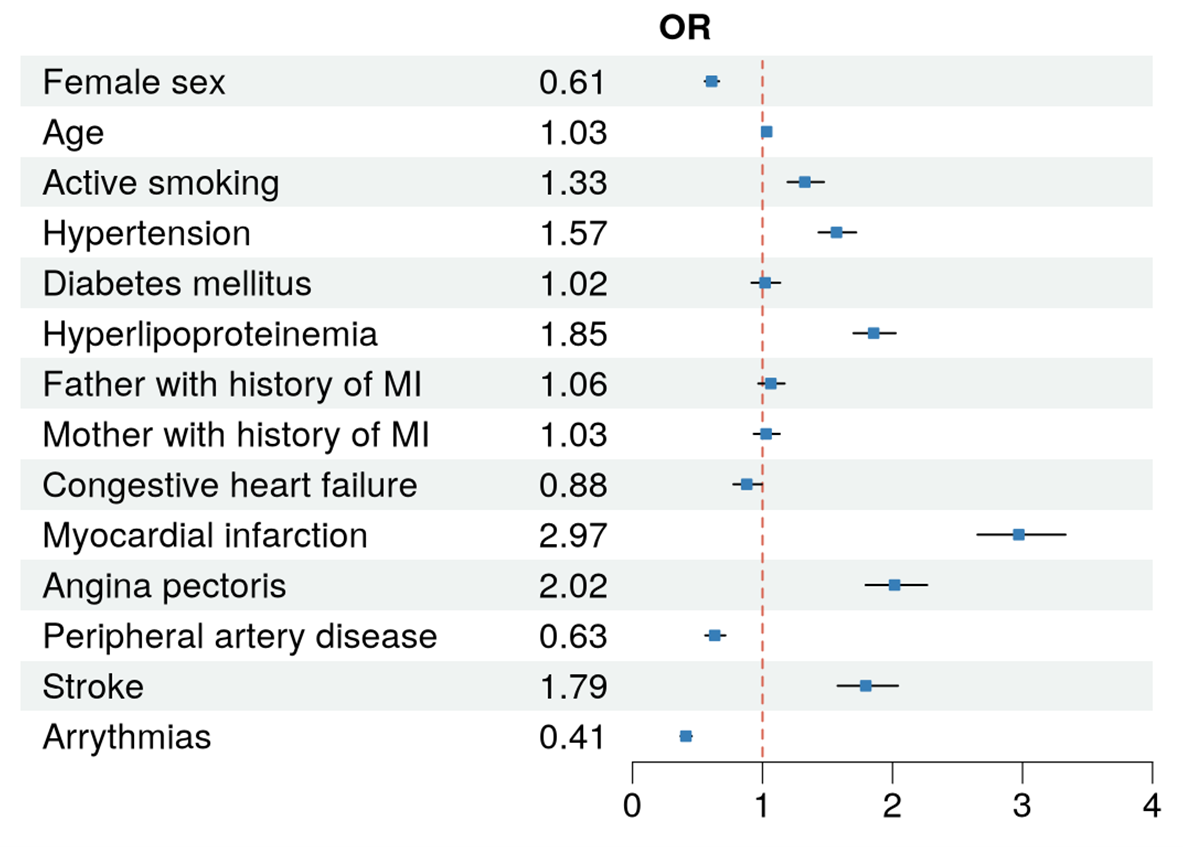
Figure 1: Multivariable logistic regression for the prediction of ASA intake in persons with cardiovascular disease