Background
Pulsed field ablation (PFA) is an innovative, non-thermal ablation technology for the treatment of atrial fibrillation (AF). Although several PFA technologies are now available, real-world and comparative data on their safety and efficacy remain limited. This study aimed to compare outcomes between the circular multielectrode array catheter (CMAC) and the variable-loop circular catheter (VLCC) in a real-world cohort.
Methods
Consecutive patients undergoing their first pulmonary vein isolation (PVI) using the CMAC or VLCC were included. All patients were prospectively enrolled in the Berlin Best-Ablate registry. All patients received PVI only under deep sedation with propofol and fentanyl. Freedom from any atrial arrhythmia was evaluated using 12-lead electrocardiography and 24-hour Holter at 6 and 12 months.
Results
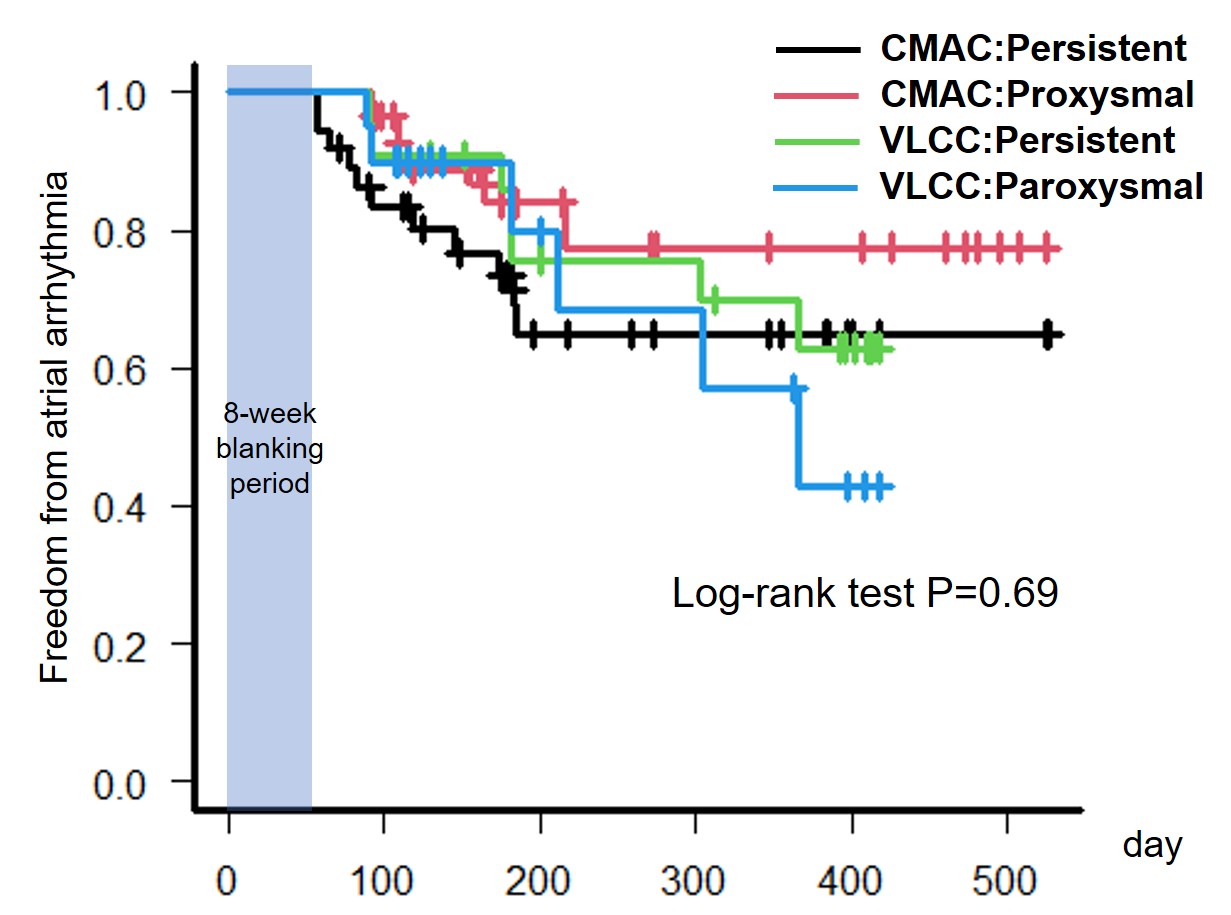
In total, 113 patients (median age; 71 [63, 77], years; 57.5% male, CMAC; 68, VLCC;45) with paroxysmal (46.0%) or persistent AF were included in this study, shown in Table 1. Patients in the VLCC group were significantly older (CMAC; 69.5 years, VLCC; 74 years, p<0.01). The proportion of AF types was comparable between the two groups (paroxysmal AF: 46.0% in CMAC vs. 45.6% in VLCC, p = 1.00). Acute pulmonary vein isolation was achieved in all patients. All procedural time metrics including procedure time, ablation time and Fluoroscopy time were longer in the CMAC group than in the VLCC group (Table 2). During a median follow-up of 182 [113–383] days, atrial arrhythmia recurrence beyond the blanking period occurred in 26.4% of all patients. There was no significant difference in recurrence rates between the CMAC and VLCC groups (23.9% vs. 31.0%, p = 0.71), shown in Figure 1. Within each group, no significant difference was observed between paroxysmal and persistent AF, illustrating in Figure 2. Two major complications (1.8%, one ischemic stroke (CMAC) and one cardiac tamponade (VLCC)) occurred.
Conclusion
In this prospective real-world study, PFA using both the CMAC and VLCC systems appeared to be effective for patients with either paroxysmal or persistent AF. There were no significant differences in atrial arrhythmia recurrence between the two PFA systems.
Table 1
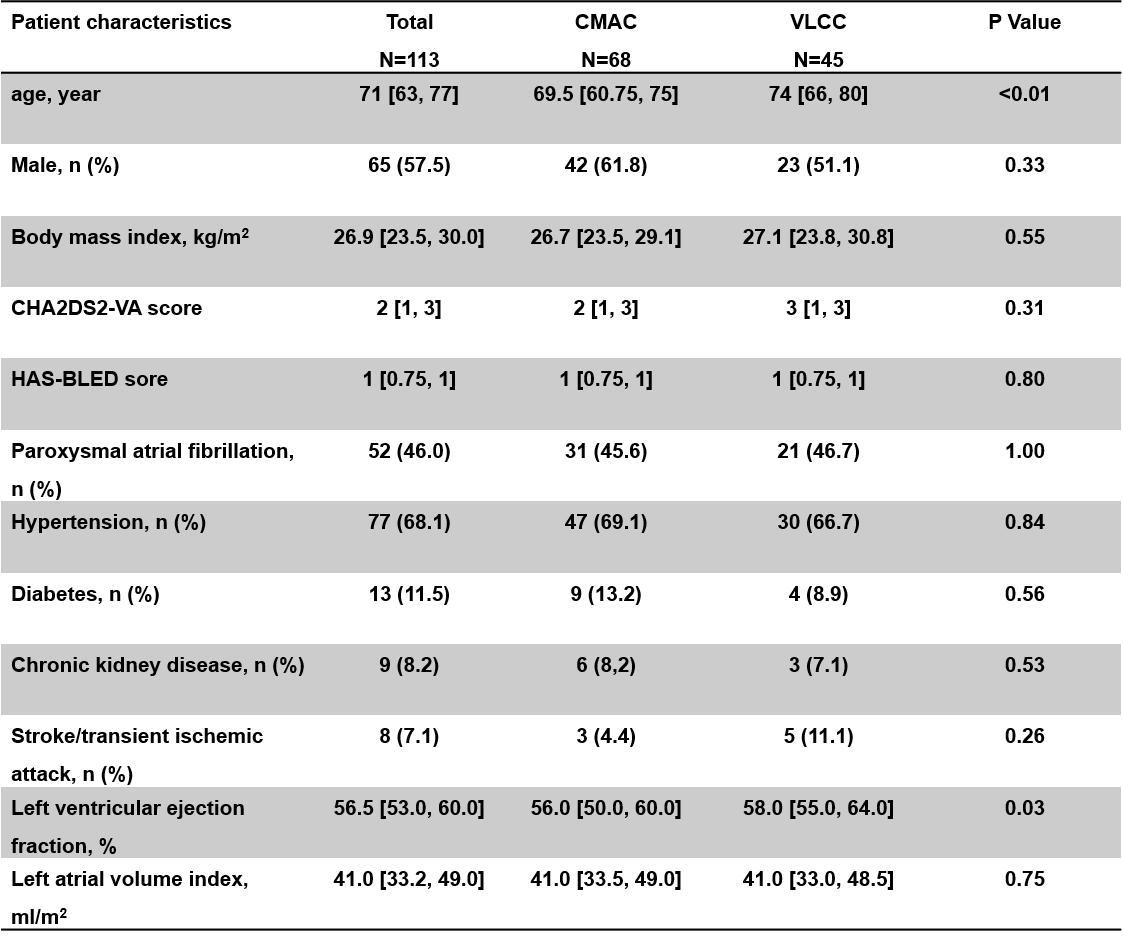
Table 2
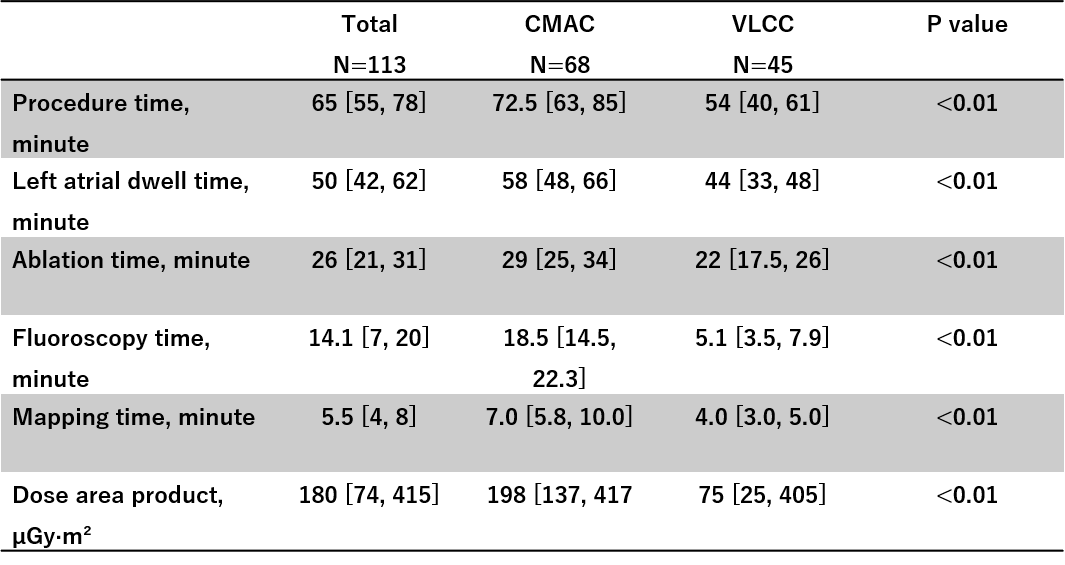
Figure 1
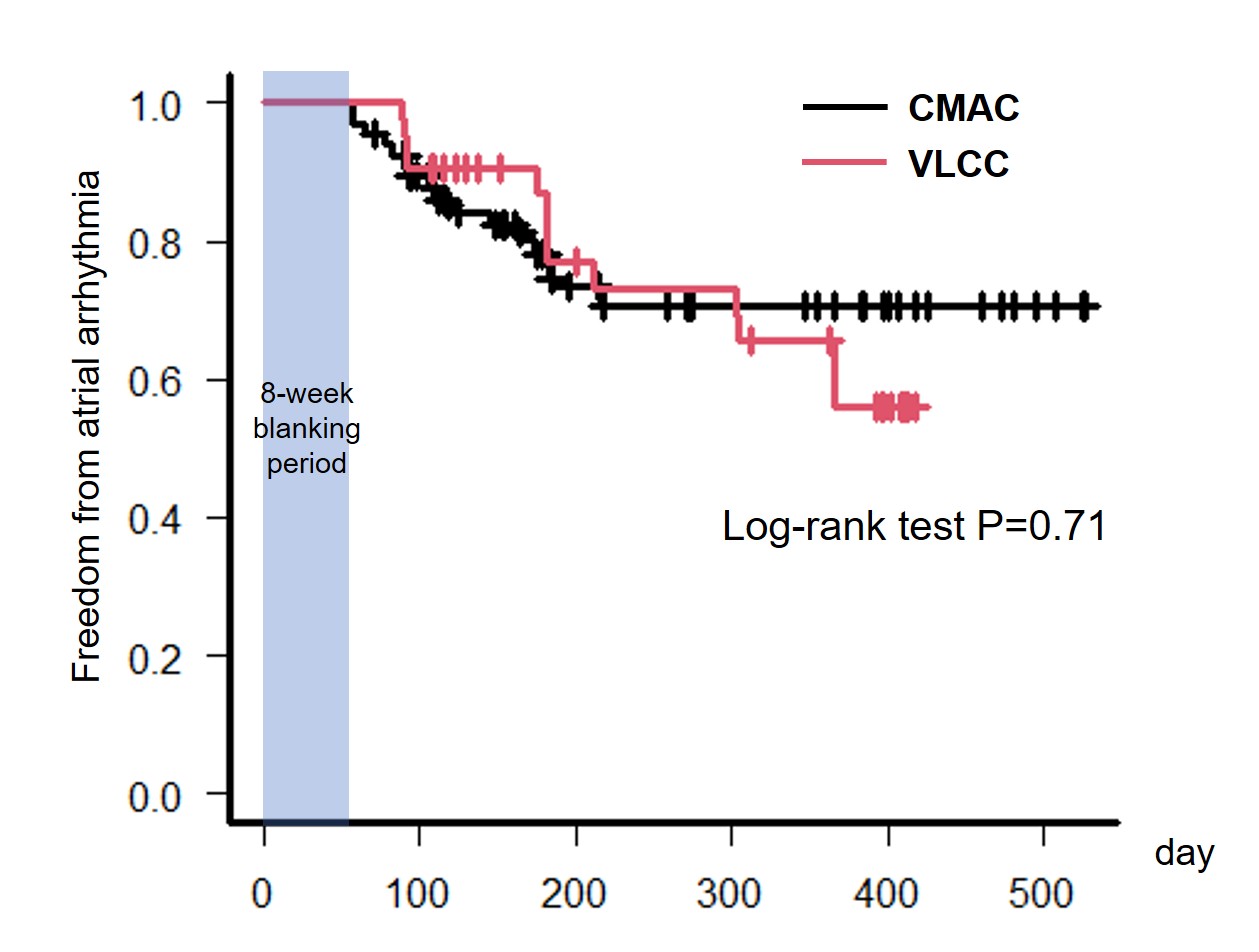
Figure 2