Background
Tricuspid valve transcatheter edge-to-edge repair (T-TEER) is increasingly established as a therapeutic option for severe tricuspid regurgitation (TR). Atrial fibrillation (AF) is highly prevalent in this patient population. However, its impact on procedural success, clinical response and survival remains unclear.
Methods
This subanalysis of the multicentre and core-laboratory adjudicated PASTE registry investigated the impact of AF on outcomes after T-TEER. The analysis compared patients with and without AF and further differentiated AF subtypes (paroxysmal, persistent, permanent). Primary endpoints were survival and clinical response, defined as improvements in NYHA class, 6-minute walk test (6MWT), and NT-proBNP. Secondary endpoints were TR reduction and intraprocedural success.
Results
1,058 patients who underwent T-TEER between February 2019 and November 2023 were included in the analysis. Of these, 961 patients (90.8%) had AF, whereas 97 (9.2%) did not. Patients with AF were older (79.7 ± 6.8 vs. 71.6 ± 13.5 years, p<0.001), had a lower baseline diuretic dose (94.1 ± 117.1 vs. 124.9 ± 172.8mg, p=0.027) and lower NT-proBNP (4,263 ± 6,136 vs. 8,018 ± 12,963pg/ml, p<0.001). They presented with larger right atria (RA area 37.7 ± 12.4 vs. 29.3 ± 8.5cm², p<0.001), lower TAPSE (17.2 ± 4.0 vs. 18.6 ± 5.6mm, p=0.003) and higher left ventricular ejection fraction (52.6 ± 11.2 vs. 49.8 ± 13.6%, p=0.026). Indexed measurements showed a larger tricuspid annulus in AF patients (22.2 ± 4.9 vs. 20.7 ± 4.3mm/m², p=0.013), while indexed RV and LV diameters were similar.
The proportion of patients in NYHA class III/IV decreased from 82.8% pre-procedure to 34.1% at follow-up, without significant differences between the groups (p=0.738). The difference-in-difference model showed no significant difference in the change of 6MWT distance (interaction p=0.392) or NT-proBNP (interaction p=0.065). At the end of the procedure, 87.7% of patients without AF and 85.7% of those with AF had residual TR ≤2+ (p=0.972). TVARC intraprocedural success was similarly high in both groups (96.0% vs. 95.9%, p=0.976). New-onset AF was documented in 14 patients (14.4%) up to 1-year follow-up.
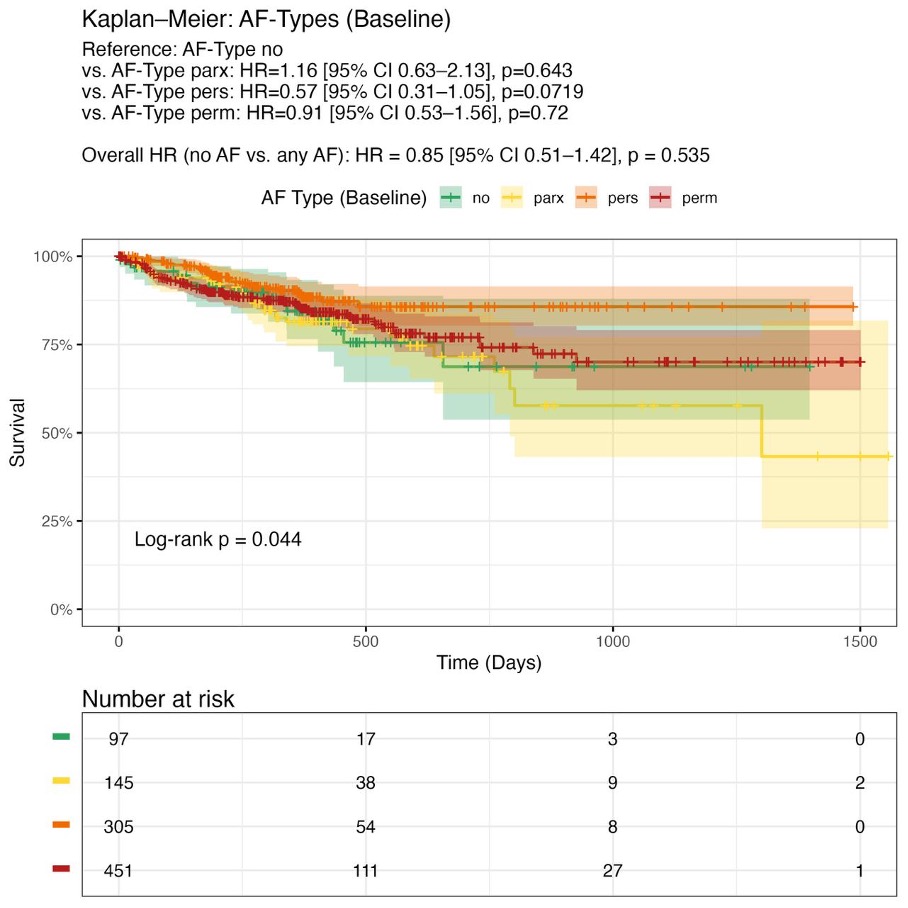
Kaplan-Meier analyses showed no significant difference in survival between patients with and without AF (HR 0.85; 95%-CI 0.51–1.42; log-rank p=0.535). In the global log-rank test, differences between AF subtypes were observed (p=0.044), which, however, was not confirmed in pairwise comparisons (paroxysmal, persistent and permanent AF vs. no AF: p=0.643, p=0.072 and p=0.720, respectively). In multivariable regression analyses, AF was not an independent predictor of either clinical response (e.g. NYHA improvement ≥1 class: OR 1.48; 95% CI 0.88–2.49; p=0.139) or survival (1-year mortality: OR 1.35; 95% CI 0.63–2.91; p=0.44).
Conclusion
AF was highly prevalent in this large, real-world cohort but had no significant impact on TVARC intraprocedural success, clinical improvement, biomarker response or survival. The potential interaction between AF and TR aetiology, as well as the role of subclinical AF and whether targeted AF therapy could further improve outcomes after T-TEER, remain to be determined.