Background
Acute kidney injury (AKI) is a frequent complication of cardiogenic shock following acute myocardial infarction (AMI-CS). The aim of the present study is to compare clinical presentation, treatment and outcomes in patients without and with AKI in a large, well-defined cohort.
Methods
Patients from three large randomized trials in AMI-CS (IABP-SHOCK II, CULPRIT-SHOCK and ECLS-SHOCK) were merged in a single database. AKI was defined according to the Kidney Disease Improving Global Outcomes criteria (KDIGO). The primary outcome was all-cause 12-month mortality. Hazard ratios were adjusted by predefined baseline and procedural caharcteristics. A step-wise logistic regression model was used to identify predictors of AKI.
Results
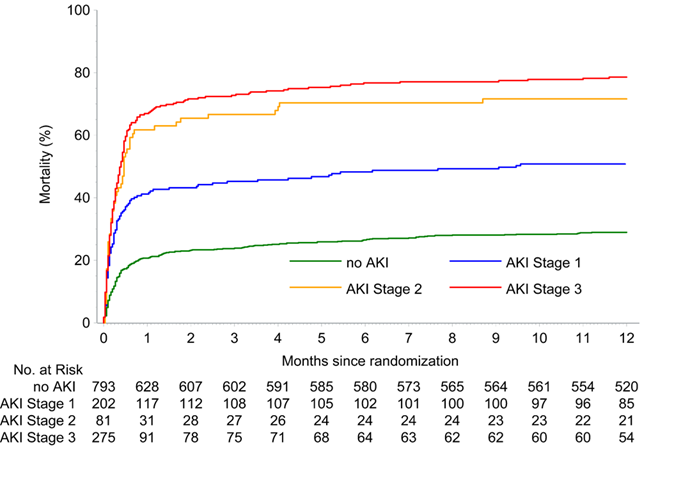
Of 1351 patients included, 793 (58.7%) did not develop AKI, whereas 558 patients (41.3%) met the definition of AKI. Of those, 249 (44.6%) needed renal replacement therapy (RRT) (18.4% of the overall population). Patients with AKI were older, had more often diabetes and known impaired renal function, as well as higher lactate levels and triple vessel disease. All-cause death at 12 months occurred in 376 of 555 patients (67.7 %) with AKI and in 230 of 790 patients without AKI (adjusted HR 3.29; 95% CI 2.79 – 3.88). Mortality for AKI stages 1, 2 and 3 was 41.3% (83/201), 61.7% (50/81) and 66.9% (184/275), respectively (Figure 1). Patients with AKI showed longer time to hemodynamic stabilization and treatment on intensive care unit, as well as higher prevalence of moderate or severe bleeding. Predictors of AKI included age, lactate levels and creatinine levels on admission, reduced flow in the infarct-related artery after revascularization, use of left-ventricular microaxial flow pump and sepsis.
Conclusion
Patients with AMI-CS and AKI displayed higher all-cause mortality at 12 months compared to those without, with increasing risks depending on AKI stage.