Background
Left ventricular ejection fraction (LVEF) often improves after transcatheter aortic valve implantation (TAVI), and early recovery of LVEF has been associated with improved long-term outcomes. Valve-in-Valve (ViV)-TAVI is increasingly used to treat degenerated bioprosthetic valves with favorable hemodynamic results; however, the evolution of LVEF after ViV-TAVI remains poorly characterized.
Aims
This study aims to evaluate the evolution of LVEF in patients with degenerated aortic bioprostheses undergoing ViV-TAVI using both conventional echocardiography and artificial intelligence.
Methods
Changes in LVEF from baseline to 3-month follow-up were retrospectively analyzed using data from a single-center German registry including 183 consecutive patients who underwent ViV-TAVI for degenerated aortic bioprostheses between 2017 and 2025. LVEF was assessed using both conventional methods and the QUEST-EF deep learning algorithm applied to two-dimensional apical four-chamber echocardiographic videos. Patients were further stratified according to the underlying mode of bioprosthetic valve failure (predominant intravalvular regurgitation (AR) vs. Restenosis (AS)).
Results
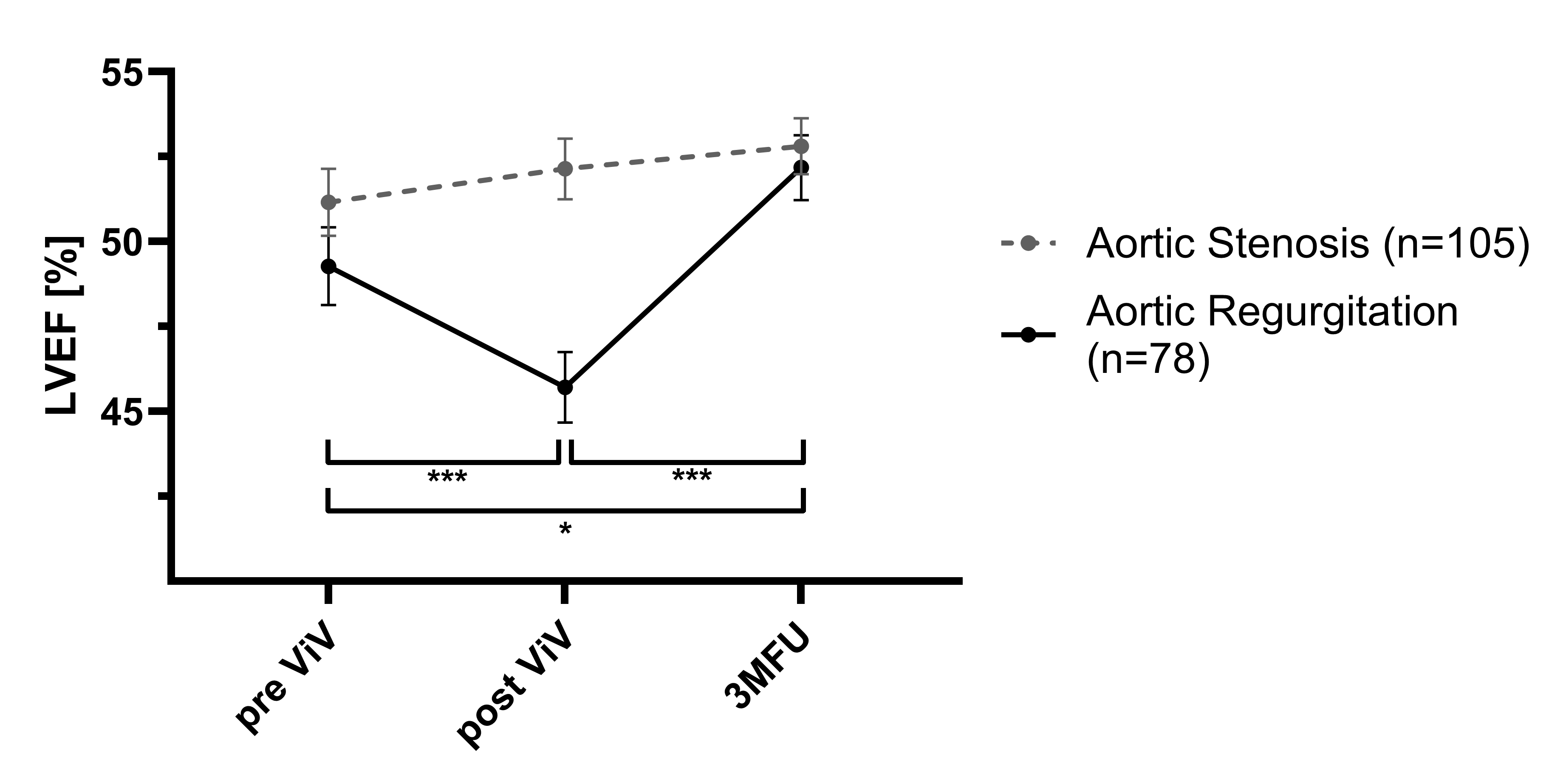
In a multifactorial analysis of variance, LVEF varied significantly over the 3-month follow-up period and between predominant AR and AS as the primary modes of bioprosthetic valve (p=0.011 F(2,180)=16.11, ηp²=0.152).
In patients with AR (n=78), LVEF showed a statistically significant transient decline immediately after the procedure (∆LVEFpre vs. post -3.57 %; p<0.001), followed by a significant recovery at 3-month follow-up (∆LVEFpost vs. 3MFU +6.47%; p<0.001).
In contrast, patients with predominant AS (n=105) exhibited stable or slight increased LVEF values without an early post-procedural drop, which did not reach statistical significance.
Conclusion
Automated deep-learning–based assessment of LVEF revealed distinct temporal recovery patterns after ViV-TAVI. Patients with predominant aortic regurgitation experienced a transient post-procedural decline in systolic function, reaching levels comparable to those patients with aortic stenosis, suggesting reversible myocardial adaptation.