Background: For the cardiovascular risk stratification of patients, the assessment of left ventricular ejection fraction (LVEF) - among other parameters - is indispensable. In clinical practice, this assessment of LVEF relies on echocardiography which is, however, resource-intensive and variably accessible. Systolic time intervals have previously been shown to correlate with LVEF. Objective: A novel single synchronized multimodal sensor (combining electrical, acoustic, impedance, and seismocardiographic signals) was used to assess the electromechanical systolic time intervals. In this study, the data generated by the novel device were correlated with echocardiographic-derived LVEF.
Methods: In a prospective single-center study, 1.095 patients (n = 545, routine evaluation, cardiology ward; n = 550, pre-operative evaluation, surgery ward) undergoing transthoracic echocardiography received parallel, synchronized recordings of ECG, impedance cardiography (ICG), phonocardiography (PCG), and seismocardiography (SCG) with one integrated device. Patients were categorized by LVEF in four groups: severe dysfunction <30%, moderate 31–40%, mild 41–51%, normal/preserved ≥52%. Extracted measures included PQ, QRS, QT/QTc; pre-ejection period (PEP); Q–S1 and Q–S2 (Q onset to first/second heart sound); Q–B and Q–C (ICG B/C points); left-ventricular ejection time (LVET; ICG B- to X-point); and the systolic time ratio (STR = PEP/LVET). Group differences were analysed with nonparametric tests; rate-dependence was addressed using QTc and STR.
Results: ECG-derived intervals showed already some discriminations: QRS widened and QTc increased (+10.4%, p<0.001) with worsening LVEF (+32%, p<0.001). Considering the electromechanical-derived intervals, Q–S1 increased by +85.8% (p<0.001) with parallel rises in Q–B (+37.4%; p<0.001) and Q–C (+15.7%; p<0.001) while Q–S2 showed a smaller prolongation (+5.6%, p<0.001). LVET shortened modestly (~4–13%), and STR increased accordingly—consistent with classical systolic dysfunction physiology.
Conclusion: This novel synchronized multimodal, electro- and mechanocardiographic sensor robustly quantified ECG and systolic time intervals and reproduced expected physiology across LVEF strata. Electromechanical intervals—especially Q–S1—showed the strongest and most consistent association with impaired LV function. Multimodal interval analysis may be a promising approach for scalable functional assessment, early detection, and longitudinal follow-up of LV dysfunction, particularly in settings where the access to echocardiography is limited.
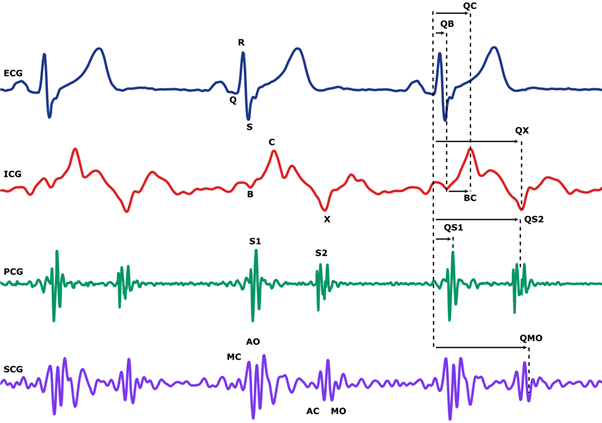
Fig 1: Diagram of the synchronous sensor signals collected by the integrated device.



