Aim: Transfemoral access is the standard route for Transcatheter Aortic Valve Implantation (TAVI), yet vascular complications remain a leading source of morbidity. Despite advances in procedural techniques and closure devices, these events persist, underscoring the need for optimal closure strategies. This study aims to compare single versus dual suture-based closure with the ProGlide/ProStyle system, focusing on vascular complications and post-procedural bleeding.
Methods: A retrospective analysis was conducted on all patients who underwent transfemoral TAVI treated with either a single or dual Pro-Glide/Pro-Style system between 2022 and 2024 at Heart- and Diabetes Center NRW (HDZ NRW, Bad Oeynhausen). Access-related vascular complications and bleeding complications were defined according to VARC-3 criteria as minor or major and categorized in a bleeding category of 1 to 4. Patients with an alternative access route, a different closure device, or aortic regurgitation as the primary indication were excluded.
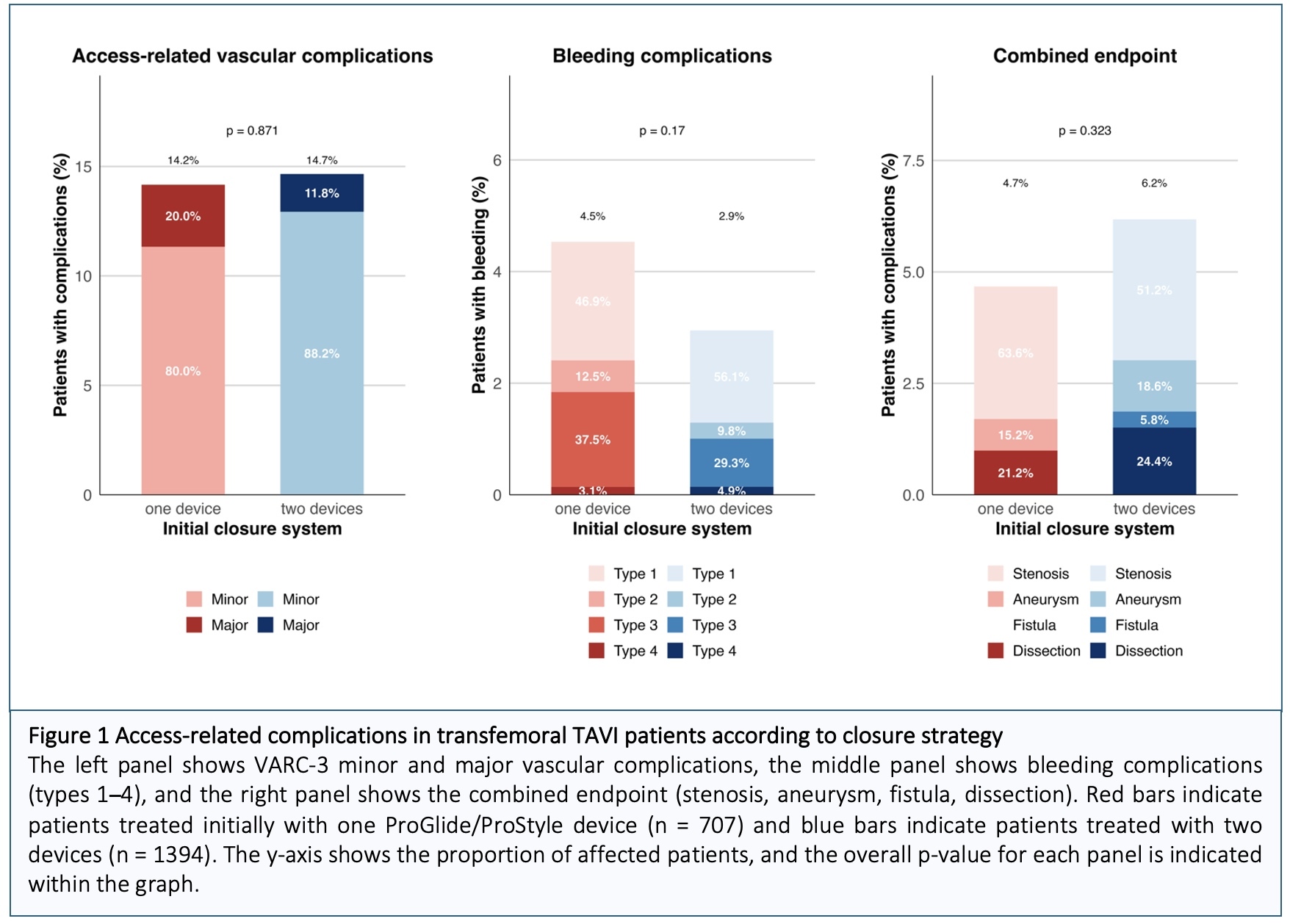
Results: The final analysis included 2,101 TAVI patients who underwent transfemoral TAVI. The mean age of the study population was 82 years, and 46.6% of the patients were female. A single ProGlide/ProStyle device was initially used in 707 patients (33.6%), while 1,394 patients (66.4 %) received two devices. An additional closure device was required in 5.4% of patients (4.8 % vs. 5.6 %; p = 0.47), most frequently plug-based systems, such as MANTA or AngioSeal. Access-related vascular complications, as defined by VARC-3, including hematoma, bleeding, stenosis, and other vascular events such as rupture, dissection, ischemia, infection, aneurysm, or arteriovenous fistula, occurred in 14.5 % of patients overall, with similar rates observed between the single-device and dual-device groups (14.2 % vs. 14.7 %; p = 0.87). The majority of these events were minor (80.0 % and 88.2 %), predominantly hematoma (8.4 % vs. 8.7 %; p = 0.879), followed by bleeding and stenosis. The distribution of vascular subtypes and the prevalence of peripheral artery disease were similar between groups (4.9 % vs. 5.5 %; p = 0.68). Bleeding complications were slightly more frequent in patients treated with a single device (4.5 % vs. 2.9 %; p=0.17); however, there was no significant difference in the need for blood transfusion (p = 0.37). Approximately half of all bleeding events were mild (VARC 3 type 1 bleeding: 37.5 % vs. 29.3 %; p = 0.49), whereas severe bleeding classified as type 4 was rare (3.12 % vs. 4.88 %; p > 0.99). The combined endpoint of stenosis, aneurysm, fistula, or dissection occurred more frequently in the dual-device group, although this difference was not statistically significant (4.7% vs. 6.2%; p=0.32).
Conclusion: Both single and dual ProGlide/ProStyle closure strategies demonstrated comparable overall VARC-3 vascular complication rates. Single-device closure was associated with slightly more bleeding, while dual-device closure showed a higher incidence of stenosis and dissection, indicating that single-device closure remains a safe and effective option for transfemoral TAVI.