Background Rotational atherectomy is an effective method for lesion preparation of severely calcified coronary artery stenoses undergoing percutaneous coronary intervention (PCI), but remains underused due to technical demands and concerns about complications. This retrospective study analyzed – periprocedural and access-associated complication rates of rotational atherectomy at a high-volume center.
Methods An all-comer cohort of 427 patients scheduled to undergo PCI with rotational atherectomy was included. Periprocedural complications were recorded in all patients in whom rotational atherectomy was actually performed, while access-related complications were recorded in all patients in whom rotational atherectomy was planned. Patients with concomitant use of a mechanical circulatory support via the femoral access route were excluded.
Results Of the 427 patients, 76.2% were male, mean age was 74 ± 8.6 years and 64.6% had coronary 3-vessel disease. The access site for rotational atherectomy was radial in 40.0% and femoral in 60.0% of patients. Sheath size was 6 Fr in 33.1% of cases, 7 Fr in 64.7%, and 8 Fr in 2.2%.
Periprocedural complications occurred in 12.9% (54/417) of patients undergoing rotational atherectomy, most often hemodynamic instability (5.8%, 24/417; figure 1). Additional complications included bradycardia in 1.7%, device complications in 1.7%, ischemic electrocardiogram changes in 1.4%, coronary artery perforations in 1.2%, no-reflow or slow-flow phenomena in 1.0% and coronary artery dissections leading to hemodynamic compromise in 0.2% (figure 1). Female sex (OR 2.337, 95%CI 1.271 – 4.297, p=0.006) and small body size (OR 0.954, 95% CI 0.923 – 0.985, p=0.004) were independent predictors of periprocedural complications. Access-related complications occurred in 9.1% (38/419) of interventions. The most common access-related complication was bleeding with 7.9% (33/419; figure 2), Independent risk factors for access-related complications were female sex (OR 3.885, 95% CI 1.962 – 7.690, p < 0.001) and small body size (OR 0.933, 95% CI 0.899 – 0.968, p < 0.001) as well as femoral vascular access (OR 3.347, 95% CI 1.438 – 7.791, p=0.002) and low body weight (OR 0.970, 95% CI 0.946 – 0.993, p=0.013).
In-hospital mortality was 1.2%, but neither periprocedural nor access-associated complications were predictors of intrahospital death.
Conclusion Periprocedural and access-related complications continue to occur relatively frequently with rotational atherectomy. However, the complications are not associated with increased in-hospital mortality. Patients with a particularly high risk of access-related and periprocedural complications are women with low body weight.
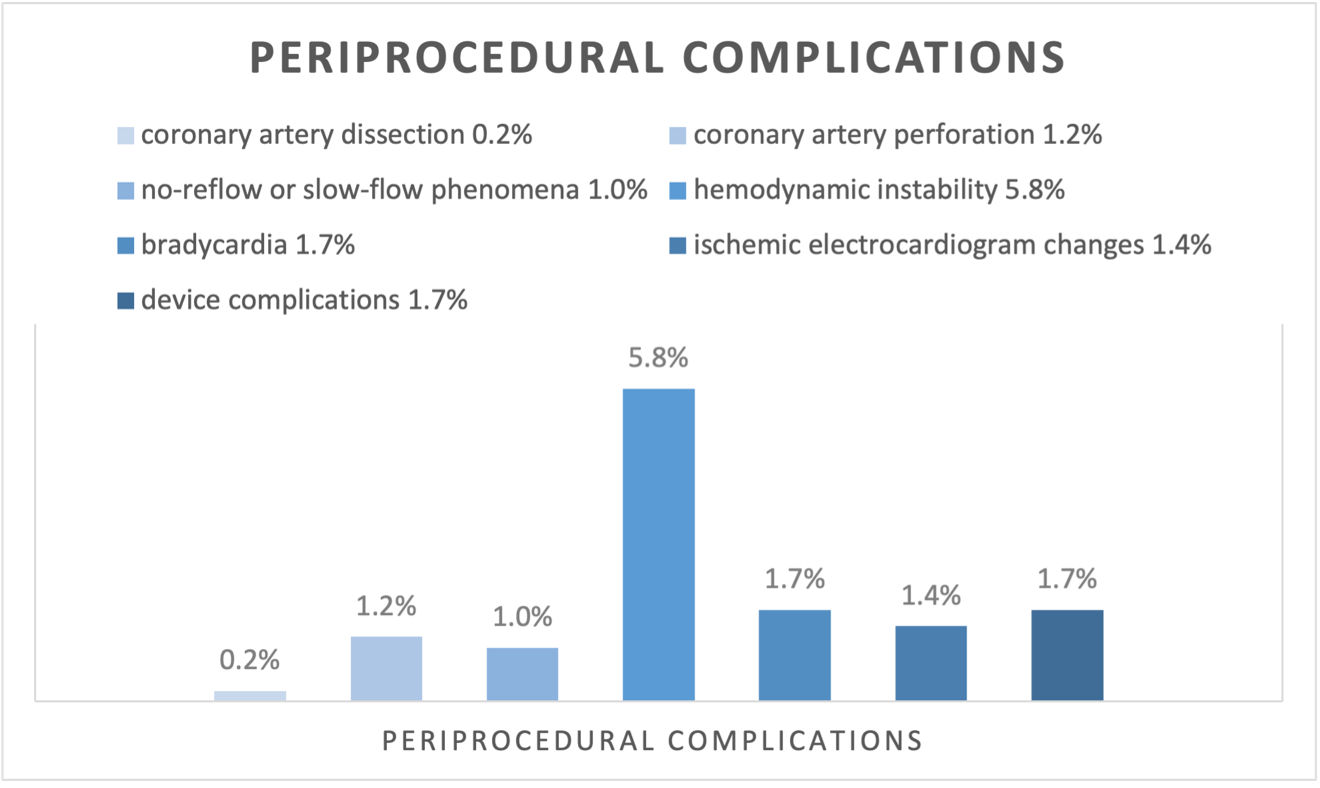
figure 1: n = 417 patients
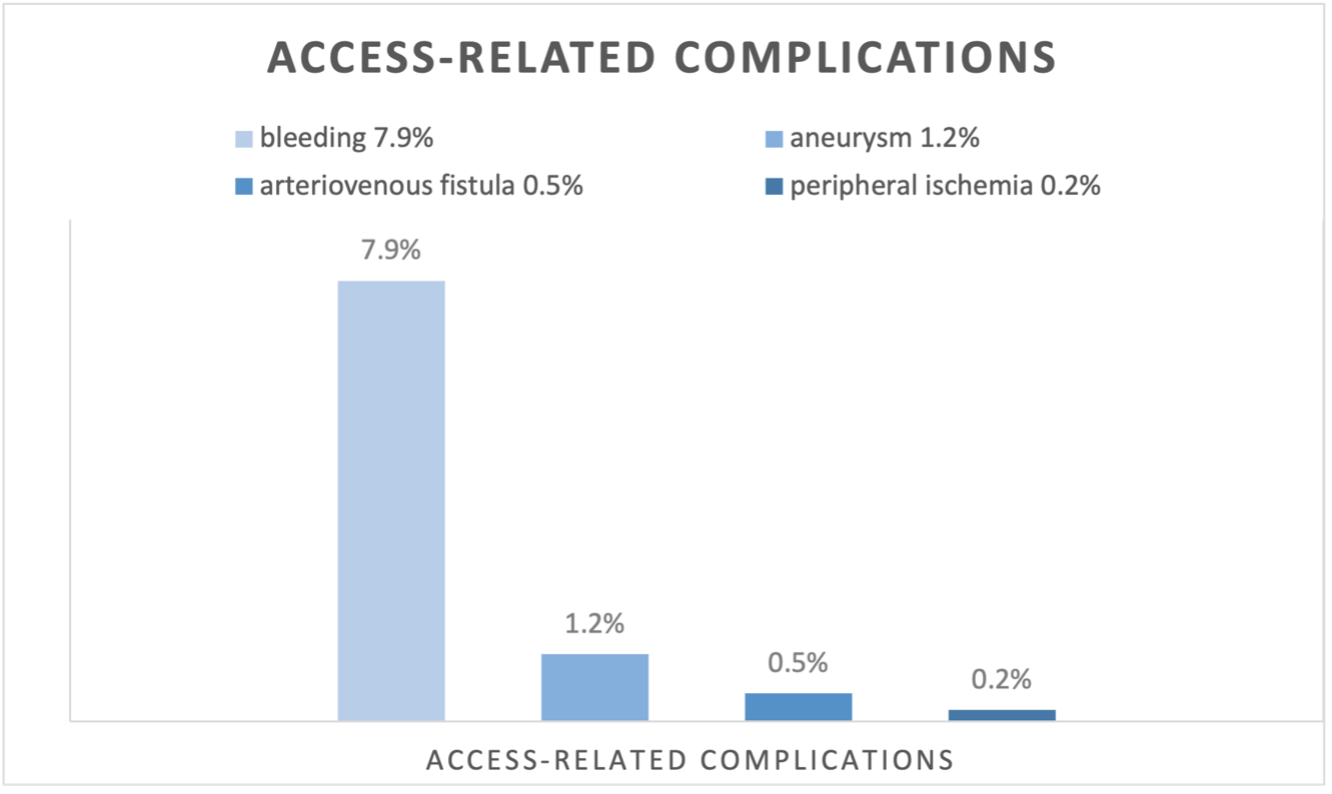
figure 2: n = 419 patients



