Background
Cardiogenic shock (CS) remains one of the most severe complications of acute myocardial infarction, carrying exceptionally high morbidity and mortality. Recent evidence from acute heart failure (AHF) cohorts suggests that transitional stages of hemodynamic instability — so-called PRESHOCK states — are associated with adverse outcomes. Whether this concept applies to ST-segment elevation myocardial infarction (STEMI), a leading cause of CS, has not been systematically investigated. Early recognition of such transitional states could offer a therapeutic window for timely hemodynamic support.
Objective
To determine the prevalence and short-term outcomes of the PRESHOCK phenotype at admission in STEMI patients, compared with those without or with criteria for shock phenotype, and to evaluate whether this admission-based phenotype predicts subsequent deterioration.
Methods
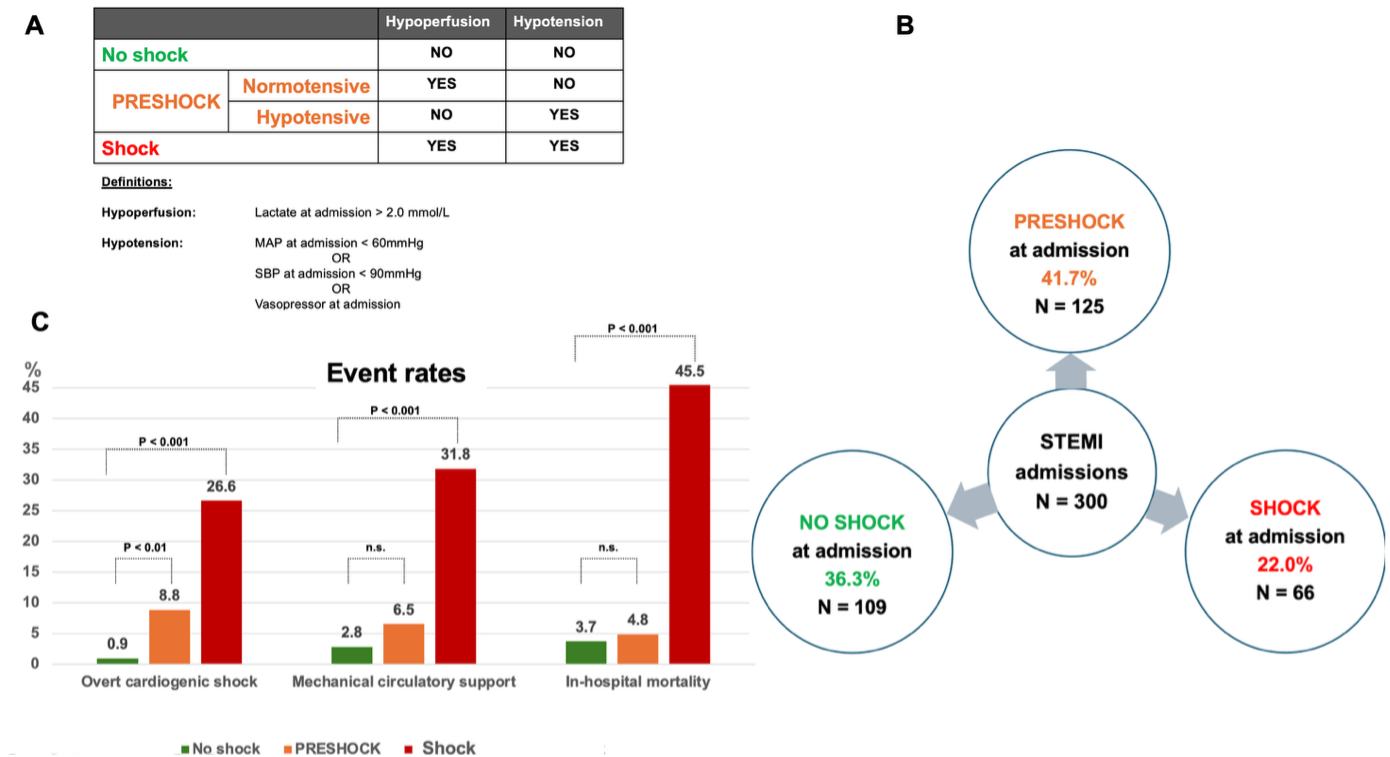
This multicentric metropolitan STEMI registry included patients enrolled between January 2024 and October 2025. Classification was derived from a single hemodynamic assessment at admission, allowing investigation of the predictive value of early hemodynamic instability for subsequent shock development (see A). Statistical comparisons used χ² or Fisher’s exact tests for categorical and Mann–Whitney U or Kruskal–Wallis tests for continuous variables. A two-sided p-value <0.05 was considered statistically significant. Investigated outcomes included overt CS (as judged by the treating physician in the context of contemporary guidelines), use of mechanical circulatory support (MCS) and in-hospital mortality.
Results
A total of 1,128 STEMI patients were recorded, of whom 300 had complete hemodynamic data and were eligible for analysis. Among these, 109 patients were classified as no-shock, 125 as PRESHOCK, and 66 as shock phenotype (see B). Within the PRESHOCK group, 108 patients had isolated hypoperfusion and 17 isolated hypotension. This corresponded to an estimated PRESHOCK prevalence of at least 11.1% in the overall registry and 41.7% in the analyzed cohort.
Baseline characteristics were similar across groups, while hemodynamic variables differed as expected. Overt CS developed in 9.8% of cases overall: 0.9% in the no-shock group, 8.8% in PRESHOCK, and 26.6% in shock group (see C, p<0.001). PRESHOCK patients showed a significantly higher likelihood of progressing to overt CS than no-shock patients (p<0.01). Even after exclusion of resuscitated cases, this finding remained roughly consistent (0.9% vs. 5.7%, p=0.053). MCS was used in 32 cases, differing overall due to the shock group (31.8%), while no-shock (2.8%) and PRESHOCK (6.5%) rates were comparable (p=0.18). In-hospital mortality was highest in shock group (45.5%), with no significant difference between no-shock (3.7%) and PRESHOCK (4.8%, p=0.66).
Conclusion
At least one in nine STEMI patients fulfilled the PRESHOCK definition at admission. PRESHOCK status identified a subgroup at increased risk of developing overt CS. Recognition of this phenotype at admission may allow proactive risk stratification and timely initiation of hemodynamic support. Future studies should further characterize the STEMI-PRESHOCK population, define optimal monitoring thresholds, and evaluate targeted therapeutic strategies to prevent progression to CS.