BACKGROUND
Multivalvular heart disease (MVHD) is common among patients with aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI). Despite growing evidence of its prognostic relevance, the interaction between biological sex and the prevalence and clinical impact of concomitant valvular disease in this population remains underexplored.
OBJECTIVE
This study aimed to evaluate the sex-specific prevalence of moderate-to-severe. In particular, we sought to assess and compare the impact of concomitant moderate-to-severe mitral and tricuspid regurgitation (MR and TR) on outcomes at 1 and 5 years after TAVI, with prespecified sex-stratified analyses to determine whether the prognostic implications of MVHD differ between women and men.
METHODS
The study cohort included 3,484 consecutive patients who underwent TAVI between 2008 and 2025 (46.1% women, 53.7% men). All patients underwent comprehensive echocardiographic assessment of valvular dysfunction and ventricular function. The primary clinical endpoint was all-cause mortality at 1 and 5 years after TAVI.
RESULTS
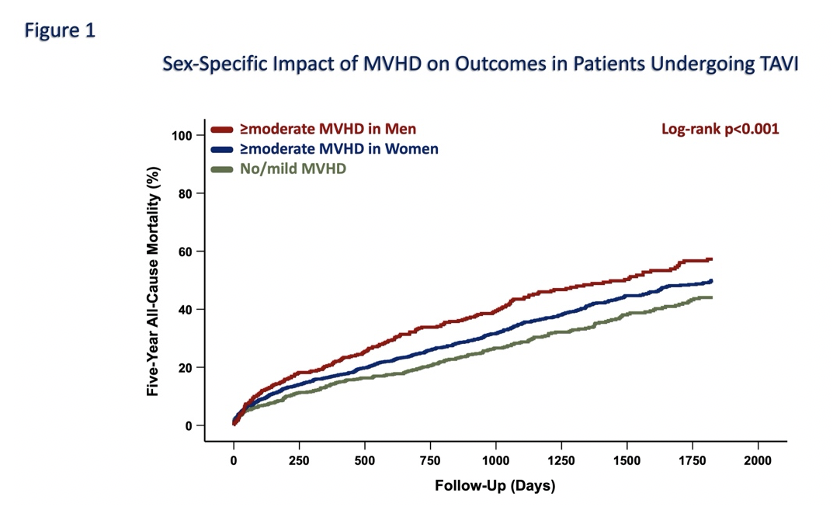
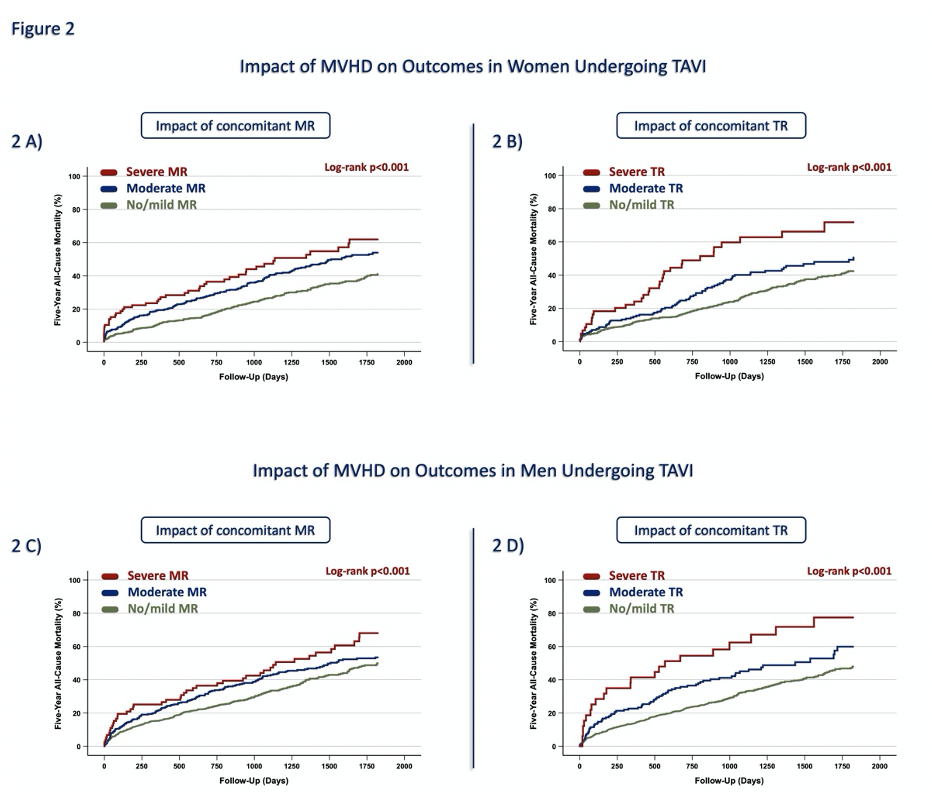
The mean age of the overall population was 80.9±6.3 years; women were significantly older than men (81.9±6.0 vs. 80.0±6.4 years, p<0.01). Concomitant MVHD was significantly more prevalent in women (≥moderate MR: 54.6% vs. 45.4%, p<0.01; ≥moderate TR: 57.5% vs. 42.5%, p<0.001). Echocardiographic analyses showed that persistent ≥moderate MVHD was associated with a more compromised hemodynamic profile, including lower left ventricular ejection fraction, higher systolic pulmonary artery pressure, and elevated NT-proBNP levels in both sexes (p<0.01). Overall, ≥moderate MVHD was associated with significantly higher 1- and 5-year all-cause mortality (14.4% vs. 9.4%, p<0.001; 37.1% vs. 22.9%, p<0.001, respectively). In the overall cohort, the highest mortality was observed in patients with ≥moderate TR, followed by those with ≥moderate MR and mild/no MVHD (p<0.01). Sex-stratified Kaplan–Meier analyses revealed that ≥moderate MVHD was associated with worse 5-year outcomes in men compared with women (p<0.001; Figure 1). Notably, ≥moderate MR was associated with similar 5-year mortality in men and women (43.0% vs. 42.2%, p=0.80), whereas ≥moderate TR was linked to significantly higher 5-year mortality in men compared with women (39.3% vs. 30.3%, p=0.05). However, increasing MR and TR severity corresponded to a stepwise decline in 5-year survival in both sexes (p<0.001; Figure 2).
CONCLUSIONS
MVHD is common among patients undergoing TAVI and occurs more often in women than in men. Although MVHD is associated with higher mortality in both sexes, men with ≥moderate MVHD experience worse 5-year outcomes, primarily driven by TR. These findings underscore the importance of incorporating sex-specific and lesion-specific factors into risk stratification and post-TAVI follow-up strategies.